

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The microvolt T-wave alternans (MTWA) test, which is based on the measurement of microvolt-level T-wave alternans beat by beat on electrocardiogram (ECG), is a non-interventional diagnostic method used to grade patients at risk for sudden cardiac death.1) Particularly, studies conducted in the last 10 years have revealed that the MTWA test is an effective method to assess patients at a high risk of arrhythmia mortality among those who had myocardial infarction (MI), ischemic or non-ischemic cardiomyopathy. The MTWA test also has very high negative predictive value for arrhythmic mortality in this subset of patients.1)2)3)
A stressed heart supplies its energy requirements through fatty acid oxidation instead of the normal route which increases the tendency for acidosis and accelerates cell death. Trimetazidine is a pharmacologic agent, which shifts the energy source from fatty acid metabolism to glucose metabolism. It shifts intracellular energy production towards glycolysis by inhibiting beta-oxidation. Metabolic activity provides additional benefits for treatment of coronary artery disease and heart failure. Its effects on ECG (i.e. MTWA) and several echocardiographic parameters related with diastolic dysfunction clinically show these beneficial effects of trimetazidine.
In this study, we investigate the efficacy of trimetazidine in combination with standard treatment on MTWA and several echocardiographic parameters in patients with stable coronary heart disease.
Subjects and Methods
One hundred patients admitted to our clinic between May 2012 and July 2013 with stable ischemic coronary artery disease who underwent either percutaneous coronary interventions (PCI) or coronary artery by-pass grafting (CABG) operations within the six months before enrolment were included as the study group. Twenty-five age- and sex-matched patients with stable coronary artery disease formed the untreated control group. Each patient was informed of the study protocol and participation consent received. Our study complied with principles of the Helsinki Declaration.
Inclusion criteria
Patients with,
1. coronary artery disease defined as ≥70% stenosis in at least one coronary artery and patients who were treated either by PCI or CABG surgeries
2. sufficient and qualified echocardiographic imaging windows
3. sinus rhythm
4. signed informed consent form
Exclusion criteria
1. History of acute coronary syndrome in the last three months
2. History of acute heart failure in the last three months
3. Complex ventricular arrhythmia and serious arrhythmia
4. History of cerebrovascular event in the last six months
5. History of cardiac surgery and/or percutaneous coronary intervention in the last 6 months
6. Primary myocardial, endocardial or pericardial diseases or valve diseases
7. Congenital heart diseases
8. Aspartate transaminase and alanine transaminase values more than three times above normal limits
10. Serious chronic lung diseases and systemic diseases
11. Not being able to tolerate the medication or having hypersensitivity to the medication
12. Noncompliance with the study protocol
13. Insufficient and unqualified echocardiographic imaging windows
After consent was received, medical history, concomitant diseases, cardiovascular risk factors, current medications were recorded and physical examination was carried out for each subject. Patients eligible for the study were assessed for clinical symptoms, physical examination findings. Further, transthoracic echocardiography, an exercise stress test and a 24-hour rhythm holter screening MTWA were performed. A baseline venous blood sample was taken before trimetazidine was added to their current standard anti-ischemic treatment. After three months of trimetazidine treatment (3×20 mg/day), symptoms, physical examination, transthoracic echocardiography, exercise stress test, 24-hour rhythm holter screening MTWA and venous blood samples were reassessed. The control group took no additional treatment in this period.
Hypertension (HT) was defined according to the Joint National Committee VII guidelines; HT was diagnosed in cases of previous antihypertensive medication or two separate measurements of >140 mmHg systolic or >90 mmHg diastolic blood pressure readings.4)
Diabetes mellitus was defined as presence of one of the following: existing diagnosis or American Diabetes Association guidelines diagnostic criteria which are: 1-HbAlc≥6.5%, 2-fasting plasma glucose (PG)≥126 mg/dL, 3-oral glucose tolerance test PG≥200 mg/dL at 2 hours, and 4-any PG≥200 mg/dL in the presence of standard symptoms.5)
Hyperlipidaemia was defined if one of the following was present: existing diagnosis or National Cholesterol Education Program Adult Treatment Panel III guidelines diagnostic criteria, which are 1-total cholesterol≥240 mg/dL, 2-triglyceride≥200 mg/dL, and 3-low density lipoprotein cholesterol≥160 mg/dL.6)
Smoking was defined as current smoking or smoking in the last year. Alcohol consumption was defined as 6 months of regular alcohol consumption.
Family history was defined as coronary heart disease before 55 years for males and before 65 years for females among first-degree relatives.
24-hour Holter electrocardiogram and microvolt T wave alternans measurement
All patients in the study were monitored pre- and post-treatment with the MARS
Holter system (GE Healthcare Inc., Milwaukee, WI, USA). Patients who have a sinus rhythm were selected for MTWA analysis. Analyses of modified moving average (MMA) based MTWA were performed using the MARS PC system (GE Healthcare Inc., Milwaukee, WI, USA) running software version 7.03. Three channel records were used for MTWA analysis and the peak difference in T wave alternans (TWA) amplitude between odd- and even-numbered beats at maximum heart rates (<120 beats/min) were calculated.
The MARS PC software (GE Healthcare Inc., Milwaukee, WI, USA) identified periods of possible TWA using the MMA algorithm, a time domain-based method that bifurcates the beat stream and generates separate moving average templates for odd versus even beats.7) Average values were updated by a weighting factor of one-eighth difference between the ongoing average and the current pair of beats. MTWA magnitude was analyzed as a continuous variable and determined every 15 s of data. An additional algorithm minimized the effects of noise and artifacts. Noise limits of 20 μV were adopted in the system configuration. Manual editing was performed if the data were ineligible due to noise or artifacts. The max MTWA value was defined as the highest TWA value in any channel. In our study, MTWA>65 μV was considered positive, based on previous reports.8)9)
Echocardiography
Echocardiographic Standard M-Mode, 2 dimensional, pulsed Doppler and tissue Doppler assessments with a Vivid -3 (GE Healthcare Inc., Milwaukee, WI, USA) brand device were performed using simultaneous ECG.
Patients were examined in the left lateral decubitus position to measure aortic root, left atrium and left ventricular diameters, as well as the left ventricular septum and posterior wall thickness on the parasternal long axis. The left ventricular end-diastolic volume and end-systolic volumes were determined on apical four-chamber plane and ejection fraction was calculated using modified Simpson’s method. Valve insufficiencies were assessed semi-quantitatively.
In pulsed Doppler assessment in apical four-chamber plane, sampling was positioned between the mitral valve edges, parallel to ventricular inflow. Subsequently peak early mitral inflow velocity (E), peak late diastolic mitral inflow velocity (A), E/A ratio, E wave deceleration time (time for E peak flow to return to baseline) were measured. Isovolumic relaxation time (IVRT) was defined as time between mitral valve opening and end of ejection.
Additionally, the device was set at tissue Doppler echocardiography (TDE) mode to measure pulse wave sample volume in apical four-chamber views and positioned at mitral lateral and septal annulus to record myocardial velocities. Systolic myocardial velocity (S’), early diastolic (E’) and late diastolic myocardial (A’) velocities were measured from septal and lateral annuli by the obtained images.
Statistical analysis
Calculations were computed on SPSS 16.0 statistical software (SPSS Inc., Chicago, IL, USA). Descriptive statistics for specified continuous variables were summarized as mean±standard deviation while categorical variables were summarized as number and percent. Paired samples t-tests were used to compare before and after differences in means for continuous variables. Chi-square tests were used to determine relationships between groups and categorical variables. Repeated measures analysis of variance with respect to the main effects of time (baseline vs. 3rd month), groups (control and trimethazidine) and the interaction between time and groups evaluated the echocardiographic parameters and MTWA values. Since our aim was to evaluate the change of variables over time between the groups, only interaction p values were presented. A two-sided p of <0.05 was considered statistically significant.
Results
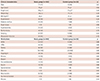
Baseline clinical characteristics of the patients are summarized in Table 1. Table 1 also shows the medications patients were using.
Table 1
Clinical characteristics and patient medications
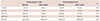
After three months of treatment, no significant change occurred in baseline echocardiographic characteristics and left ventricular systolic functions in both groups (Table 2). Mean left ventricular end-systolic volume, left ventricular end-systolic diameter, mean left ventricular end-diastolic volume, end-diastolic diameter and left atrial volume did not change after treatment (Table 2). Table 3 summarizes the left ventricular diastolic functions, which were assessed by echocardiography. After three months of treatment, significant improvement only in IVRT was found in the study group (Table 3).
Table 2
Effects of trimetazidine on parameters of left ventricular structure and systolic function

AoD: aortic root diameter, LAD: left atrial diameter, LVEDD: left ventricular end-diastolic diameter, lVESD: left ventricular end-systolic diameter, IVSD: interventricular septum diastolic dimension, PWD: posterior wall dimension, EF: ejection fraction, LVEDV: left ventricular end-diastolic volume, LVESV: left ventricular end-systolic volume, LAV: left atrial volume
Table 3
Effects of trimetazidine on parameters of left ventricular diastolic function
Regarding TDE parameters of the study group, no significant difference was observed except for in the lateral annular early diastolic myocardial velocity (E’ lateral) and Septal annular systolic myocardial velocity (S’ septal). E’ lateral and S’ septal increased significantly after three months of treatment with trimethazidine. Further, left ventricular end-diastolic filling pressures showed no significant differences (Table 4).
Table 4
Effects of trimetazidine on parameters of left ventricular tissue Doppler echocardiography

TWAmax values significantly reduced after trimethazidine treatment (Table 5) in the study group. Moreover, abnormal MTWA test results significantly improved after three months of trimetazidine treatment.
Table 5
Effects of trimetazidine on T wave alternans

Discussion
In our study, we investigated the effects of trimetazidine on MTWA, a non-invasive predictor of sudden cardiac death and several echocardiographic parameters in patients with stable coronary artery disease.
Herein, we found that MTWA test significantly improved after trimetazidine treatment for three months. MTWA test, which is based on measurement of microvolt-level T-wave alternans beat by beat on ECG, is a non-interventional diagnostic method used to grade patients at risk for sudden cardiac death. Particularly, studies conducted in the last 10 years have revealed that the MTWA test is an effective method to identify patients at high risk for arrhythmia mortality among those who had MI or ischemic or non-ischemic cardiomyopathy. In other disease states like vasospastic angina, MTWA testing has been used as a predictor for arrhythmic complications.10) This test is a marker of electrical instability and our study is the first to show MTWA parameter improvement after trimetazidine treatment.
Further, we found that trimetazidine improved several echocardiographic parameters related to diastolic dysfunction. Vitale et al.11) found that diastolic function improved after six months of trimetazidine treatment, with significantly increased E/A and decreased atrial deceleration time, IVRT and pulmonary vein systolic velocity waves. In our study, IVRT decreased and E’ lateral increased significantly.
In a study by Fedorova et al.12) with a beta blocker and trimetazidine combination treatment, advanced functional class heart failure patients showed a 59% reduction in E/A ratio after six months follow-up. However, these patients had a restrictive filling pattern and had shorter deceleration time and IVRTs. In our study, we determined a significant reduction in IVRT, which is in concordance with that study. The metabolic effects of trimethazidine may take part in diastolic function improvement. However, a three-month follow-up study as our current one may be too short a time to show the beneficial effects of trimethazidine on left ventricular diastolic functions assessed by echocardiography.
In our study, the effect of trimetazidine on systolic functions by left ventricular ejection fraction was also investigated and a non-significant increase in ejection fraction (EF) was observed. Belardinelli et al.13) investigated benefits of trimetazidine in context of chronic ischemia, clinically and echocardiographically, to find that three months of trimetazidine treatment result in a 14% EF increase in diabetic ischemic heart failure patients. This effect was related to the degree of perfusion impairment determined by scintigraphy. Improvements in the left ventricular EF, clinical state and reduction in chest pain frequency were established at the end of six months of follow-up of 60 ischemic cardiomyopathy patients receiving trimetazidine.14) It was found that treatment benefits were proportional to the degree of perfusion impairment reversibility; therefore, higher benefits for impairments that are more serious. We found no significant increase in EF and assume it is related to the EF which is more than 40% in all the control group and in 96% of the study group.
Following acute myocardial infarction, patients often experience a progressive deterioration in left ventricular functions, which leads to marked heart failure. This phenomenon, described as ventricular remodelling, is not well defined and does not have a specific treatment. Combined activation of the sympathetic nervous system along with renin-angiotensin system, hypertension, hyperglycaemia and insulin resistance are suggested to be responsible for left ventricular remodelling.15)
In cases of >15% reduction in left ventricular volume, depending on the treatment regimen, reverse modelling is considered.16) In a study on trimetazidine, significant reduction in left ventricular end-systolic volume was observed after 12-18 months of treatment.17) Likewise, in our study, significant reduction was observed after three months of trimetazidine treatment. This implies that trimetazidine can have an effect on reverse remodelling.
TDE measured annular S’ is an important parameter to assess left ventricular systolic functions, in addition to parameters such as EF, wall motion scoring index, and pulse volume.18) Regional myocardial systolic and diastolic velocities are assessed by TDE.19) In recent years, it was shown that septal S’ is positively related to EF. Mitral E’ and A’ wave velocities measured by TDE are slightly influenced by pre-load and left atrial pressures. Most importantly, diagnostic value and relation to mortality of these parameters in heart failure and consequently TDE’s role in detecting cardiac functions in heart failure patients has increased.20) Progressive systolic and diastolic abnormalities lead to progressive reduction in TDE velocities.21) Myocardial velocities are related to functional capacity. Specifically, septal S’ wave velocity is closely related to functional capacity compared to standard echocardiography or TDE parameters.13) In our study, E’ lateral and S’ septal TDE parameters significantly increased after three months of treatment. Other TDE parameters showed no significant change.
Limitations
There are several limitations of the current study. First, the study population can be regarded as a low-risk population. A larger population and a longer follow-up time is necessary to show the effects of drugs on arrhythmic complications. The power of our study, in this regard, is low; however, we showed improvements in left ventricular functions and MTWA. Another limitation was that we did not perform ischemia testing before inclusion, which might have a negative effect on study parameters if present; however, our patients were asymptomatic with a good functional class and were thought to be ischemia free.
Conclusion
Trimetazidine, a metabolic regulator in myocytes, improves MTWA, a non-invasive predictor of electrical instability. In addition, several echochardiographic parameters related with left ventricular functions also improved. Thus, we conclude that trimetazidine may be an effective agent to prevent arrhythmic complications and improve myocardial functions in patients with stable coronary artery disease.
 XML Download
XML Download