

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The benefits of statin for the primary and secondary prevention of coronary artery disease are well established.1)2)3)4)5) These benefits can be obtained through the reduction of low-density lipoprotein cholesterol (LDL-C) and an increase in high-density lipoprotein cholesterol (HDL-C). Usually, statin treatment is associated with modest elevation in HDL-C; however, the HDL-C response to any given statin has a wide variation from study to study.
High-density lipoprotein (HDL) particles exert various effects, depending on their properties.6) There are both functional and dysfunctional HDL particles, and it is important to promote the functional HDL activities, including reverse cholesterol transport, anti-oxidative and anti-inflammatory actions. Oxidative modification of low-density lipoprotein (LDL) particles was a key event in atherosclerotic lesion formation. In the past few decades, it has become evident that HDL particles have antioxidative properties that protect LDL particles from oxidation. During this process, the HDL-associated enzyme paraoxonase 1 (PON1) has been suggested as a possible mechanistic cause of this phenomenon.7) Epidemiological studies indicate that high PON1 activity is inversely associated with the progression of atherosclerosis, and reduction in the incidence of coronary artery disease.8)
In our previous study, we have shown that many patients showed decreased HDL-C response after statin therapy, although the mean HDL-C of total patients was increased.9) In addition, statin-induced HDL-C changes did not predict long-term outcomes. Therefore, our hypothesis was that functional properties of HDL particle were not correlated with HDL-C levels. We compared anti-oxidative activity between the patients with increased HDL-C and those with decreased HDL-C response after statin therapy, to define functional response beyond HDL-C levels. In this study, we examined the on-treatment lipid levels and anti-oxidative properties using PON1 activity at baseline and at 8 weeks after rosuvastatin 10 mg treatment.
Subjects and Methods
Study population
This was a prospective study protocol. We enrolled and analyzed 240 statin-naive patients with stable ischemic heart disease. Exclusion criteria were acute coronary syndrome, including myocardial infarction within 3 months; no significant coronary lesions; allergy to statin; administration of drugs that can affect lipid levels including fibrate, fish oil, niacin, ezetimibe or probucol; known inflammatory, neoplastic, or infectious diseases. The patients who underwent percutaneous coronary intervention were included; however, patients who developed periprocedural myonecrosis were excluded.10) All patients provided informed consent for processing their anonymous data according to a protocol approved by the Institutional Review Board of Wonkwang University Hospital (WKUHIRB-1459).
Rosuvastatin (10 mg; Crestor®, Zoetermeer, Zuid-Holland, Nertherlands) was administered after enrollment. During the 8-weeks treatment, no patients withdrew from the study due to adverse effects of statin. Angiotensin-converting enzyme inhibitors, beta blockers, and nitrates were prescribed according to the physician's discretion.
Lipid analysis and paraoxonase 1 activity
Total cholesterol, triglycerides, and HDL-C were measured using an enzymatic colorimetric assay (Roche Diagnostics, Indianapolis, IN, USA), after 12 h overnight fasting. LDL-C was directly measured. Lipid and lipoprotein levels were obtained at baseline and at 8 weeks treatment.
PON1 activity of the serum samples was measured using full automated paraoxonase activity measurement kit (Mega Tip, Gaziantep, Turkey) on Hitachi 7600 automatic biochemical analyzer (Hitachi, Tokyo, Japan).11)
Statistical analysis
All measurements were represented as mean±standard deviation or absolute number (percentage). The patients were divided into two groups according to the changes in HDL-C: increased HDL group [on-treatment HDL-C≥baseline HDL-C], and decreased HDL group [on-treatment HDL-C<baseline HDL-C]. Inter-group analysis was performed using independent t-test and χ2 test, which were conducted using SPSS 19.0 for Window (SPSS Inc., Chicago, IL, USA). To compare the change of lipid profiles and PON1 activity before and after rosuvastatin treatment, we used paired t test. Relationships between changes in HDL-C and PON1 activity were measured by Pearson correlation coefficients. Statistical significance was set at p<0.05.
Results
Baseline characteristics
Mean on-treatment HDL-C levels were 46.2±10.1 mg/dL, and mean on-treatment LDL-C levels were 65.5±23.4 mg/dL. Rosuvastatin treatment increased the mean HDL-C concentration by 1.9±9.2 mg/dL (6.4±21.4%). HDL-C levels increased in 138 patients (57.5%), but decreased in 102 patients (42.5%) after statin treatment.
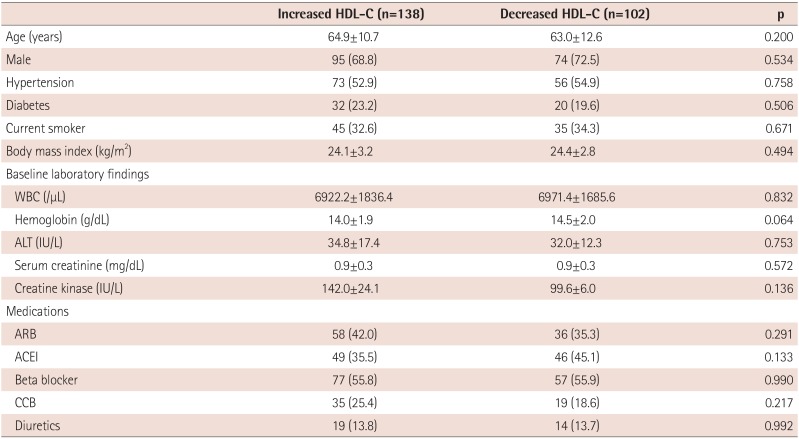
The baseline clinical characteristics according to HDL-C response are shown in Table 1. There was no significant difference in the most relevant clinical characteristics between the two groups.
Table 1
Baseline clinical characteristics
Changes of lipid and lipoprotein
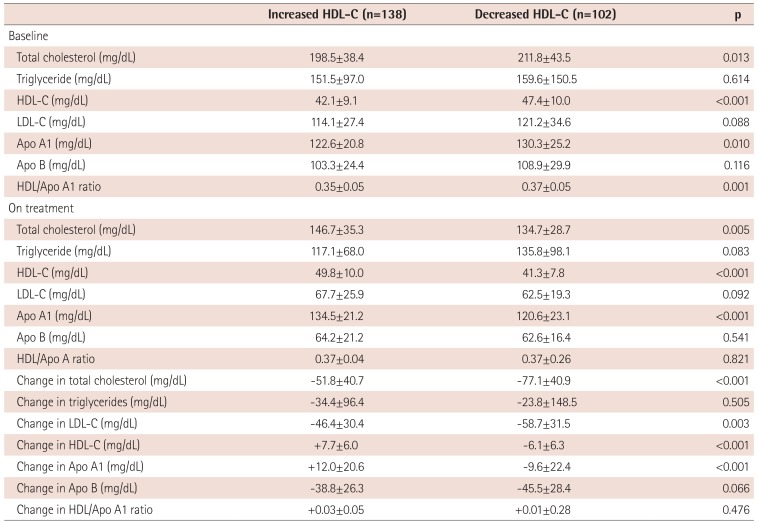
Total cholesterol, triglyceride and LDL-C levels decreased after statin treatment (Table 2). Baseline HDL-C levels were higher in patients with decreased HDL-C at 8 weeks (47.4±10.0 vs. 42.1±9.1 mg/dL, p<0.001). Baseline Apolipoprotein (Apo) A1 also higher in decreased HDL-C responder (130.2±25.2 vs. 122.6±20.8 mg/dL, p=0.010). HDL-C/Apo A1 ratio was different in both groups at baseline, but on-treatment HDL-C/Apo A1 ratio was similar: 0.01 to 0.03 increase was seen in both groups.
Table 2
Lipid findings after statin treatment
Changes of paraoxonase 1 activity
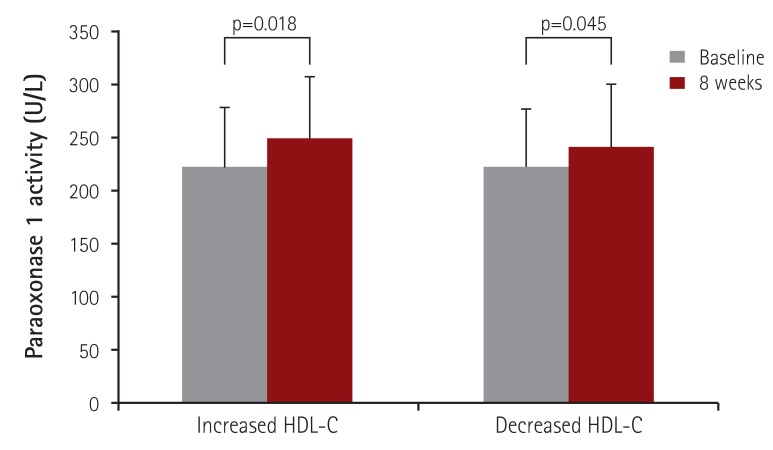
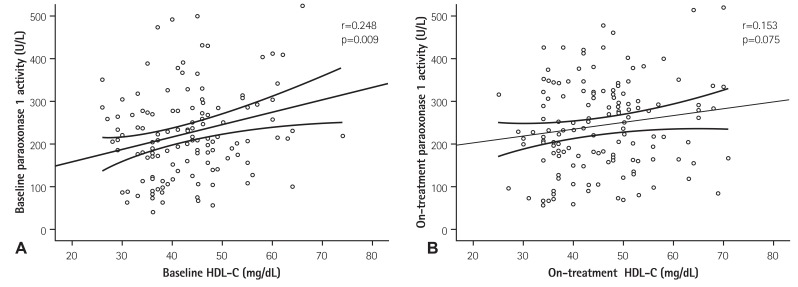
PON1 activity increased to 19.1% in all patients. In both, the patients with increased HDL-C and with decreased HDL-C, baseline PON1 activity was similar between the two groups (223.8±105.3 vs. 223.7±105.9 U/L, p=0.994), and PON1 activity significantly increased after rosuvastatin treatment (+19.3% in increased HDL-C responder; p=0.018, +18.8% in decreased HDL-C responder; p=0.045 by paired t-test) (Fig. 1). Therefore, on-treatment PON1 activity was similar between the two groups (247.8±102.3 vs. 242.6±106.9 U/L, p=0.751). Baseline PON1 activity modestly correlated with HDL-C levels (r=0.248, p=0.009); however, on-treatment PON1 activity did not correlate with HDL-C levels (r=0.153, p=0.075) (Fig. 2).
Discussion
The main findings of the present study were as follows: (1) some patients showed decreased HDL-C levels after rosuvastatin treatment, despite their overall HDL-C elevation; (2) antioxidative property assessed by PON1 activity improved after rosuvastatin treatment regardless of HDL-C levels. These observations might support that on-treatment HDL-C levels alone was not an important target in patients with ischemic heart disease.
HDL-C is a well-established risk factor for coronary heart disease (CHD). However, on-treatment values of HDL-C after statin treatment have been inconsistently correlated with the risk of cardiovascular events. High dose statin studies, such as Analyses of the Pravastatin or Atorvastatin Evaluation and Infection Therapy trial and Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial, reported that HDL-C concentrations were not predictive of residual CHD risk among patients treated with potent statin therapy who attained very low concentrations of LDL-C.12)13) The studies of HDL-C elevating drug also demonstrated that niacin or cholesterol ester transport protein inhibitors did not improve outcomes, in spite of marked HDL-C elevation in patients who underwent statin treatment.14)15) In addition, the authors previously reported that statin-induced HDL-C changes did not predict 12-months major adverse outcomes, despite more than 4% of HDL-C elevation after rosuvastatin 10 mg treatment.9)
The possible explanations about low predictive power of rosuvastatin-induced changes in HDL-C, or on-treatment HDL-C on cardiovascular outcomes, will be made by concept of HDL particle or HDL functionality. A sub-analysis of JUPITER study demonstrated that HDL particle number may be a better marker of residual risk than chemically measured HDL-C or Apo A1.16) That is, among placebo-allocated patients, the on-treatment HDL particle measured by nuclear magnetic resonance spectroscopy and HDL-C had similar inverse association with cardiovascular outcomes. However, among rosuvastatin-allocated patients, on-treatment HDL particle had stronger association with outcomes, rather than HDL-C. The number of HDL particle could be measured by HDL-C/Apo A1 ratio, indirectly.17) As the particle size of HDL increased, the HDL particle contained more Apo A1 molecules; therefore, HDL-C/Apo A1 ratio showed a linear correlation with HDL particle number. In this study, as the HDL/Apo A1 ratio increased in both groups, it indicated that HDL particle number could be increased after rosuvastatin treatment regardless of on-treatment of HDL-C levels.
Ordinary HDL particle is “functional HDL” which exerts anti-atherosclerotic, anti-inflammatory and anti-oxidative effects. When various factors such as metabolic syndrome, smoking, or chronic inflammatory conditions influence the HDL particles, they are modified from “functional HDL” to “dysfunctional HDL”.6) Statin may improve the functionality of HDL particle, especially the cholesterol efflux and anti-inflammatory action. Statin may also improve the anti-oxidative action of HDL particle via PON1.18)19)20) PON1 is an enzyme hydrolyzing peroxidized lipids, which is synthesized in the liver and is present in blood bound to Apo A1 of HDL particles.21) PON1 exerts its anti-oxidative action by inhibiting the oxidation of LDL and even HDL itself, depending on the degree of its activity.22) Statin treatment increased the PON1 activity about 10-35%.20) However, changes of PON1 activity according to HDL-C levels during statin treatment have not been demonstrated. In this study, rosuvastatin treatment significantly increased the PON1 activity to 19%. Moreover, we demonstrated that increased PON1 activity was not associated with on-treatment HLD-C levels. Therefore, HDL-C levels are not correlated to HDL functionality, especially in rosuvastatin treated patients.
Our study has several limitations. We did not evaluate cardiovascular outcomes in the study population. Clinical significance of HDL/Apo A1 ratio or PON1 activity was still unknown in rosuvastatin treated patients with stable ischemic heart disease. It is unknown whether the HDL-C response to statin is similar to that of other types of statins or of other rosuvastatin doses. Further studies would be necessary.
In conclusion, rosuvastatin treatment improved the lipid profile and anti-oxidative property assessed by PON1 activity in patients with stable ischemic heart disease. Moreover, PON1 activity was not associated with on-treatment HDL-C levels.
 XML Download
XML Download