

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Although cardiovascular disease (CVD) has been one of the leading causes of death in most developed countries, the rates of morbidity and mortality associated with CVD have been steadily decreasing during the recent decades. On the contrary, the rates of morbidity and mortality related to CVD have been rapidly increasing in Korea.1)2) Considering that the rates of other risk factors are being reduced and more controlled than before, this might be mainly due to the unhealthy lifestyle of Koreans and the associated disease of dyslipidemia. For Koreans, therefore, lifestyle modification and the management of dyslipidemia are very important in order to prevent CVD or its recurrence.
The Korean Society of Lipidology and Atherosclerosis and other related societies and organizations came together and formed the Committee for the Guidelines for the Management of Dyslipidemia, to provide opinions for the proper management of dyslipidemia with the aim of preventing CVDs in Korea. We published the first edition of the Guidelines for the Management of Dyslipidemia in 1996 and the second edition in 2003. New guidelines for dyslipidemia management were published in Europe (2011) and in the United States (2013), on the basis of the most recent research results.3)4) In this regard, 18 related societies and organizations in Korea gathered to suggest new guidelines for dyslipidemia management.
Appropriate guidelines should be established on the basis of individual evaluations of the future risks of CVD and death. This risk evaluation is possible only if the potential risk factors can be accurately estimated in a representative Korean population followed up for a long term and, at the same time, if the rates of CVD and death are precisely recorded. Although several studies have been published in Korea, it might be difficult to apply the results to actual clinical practice owing to the lack of the above-mentioned elements.5) In addition, it is not possible to quote Western risk evaluation criteria, as the mortality of ischemic heart disease in Korea is among the lowest worldwide.
In this background, we adopted the previous approach, instead of following the trends of overseas treatment guidelines. There is a desperate need, at this time, for a study to evaluate the risk of CVD in Koreans. In addition, almost all studies on the management of dyslipidemia are from Western countries, and a review of those studies is necessary to determine whether such results can be applicable to Koreans. The grade of recommendation and the evidence level in this treatment guideline were quoted from the treatment guidelines of the American College of Cardiology and the American Heart Association (ACC/AHA).4) For more details, it would be helpful to see the full text, which will be published along with a summary.
Korean guidelines for management of dyslipidemia were made in full text and in executive summary. And this is the English translation version of the executive summary. This treatment guideline was based on observatory studies that investigated the preventive effects of dyslipidemia management. Therefore, it does not mean that this guideline should be applied to all patients with dyslipidemia. Instead, physicians should make their final decision about how to treat their patients on the basis of the clinical judgments.
Chapter 1. Epidemiology of Dyslipidemia in Koreans
1. Current status of cardiovascular disease in Korea
Annually, 17000000 people die of CVD worldwide, which accounts for 30% of all deaths.6) In Korea as well, CVD is one of the leading causes of death, where the mortality of coronary artery disease (CAD) was 31 per 100000 males and 27 per 100000 females in 2012 (Fig. 1-1), whereas the mortality of cerebrovascular diseases was 49 per 100000 males and 53 per 100000 females in the same year (Fig. 1-2). Nevertheless, mortality from cerebrovascular diseases has greatly decreased since the 1990s, whereas that from coronary artery disease (CAD) has recently begun to slightly decrease when adjusted for age (Fig. 1-1).
For cerebrovascular diseases, whereas more people died of cerebral hemorrhage (nontraumatic intracerebral hemorrhage and subarachnoid hemorrhage) before 2002, death due to cerebral infarction (ischemic stroke) predominated since 2002 (Fig. 1-3). This might be due to the improved management of blood pressure, thereby reducing events of cerebral hemorrhage, and the better treatment for cerebral hemorrhage.
Compared with the mortality data, it is difficult to identify such changes in the prevalence and incidence rate of CVD, owing to the lack of nation-wide statistics.
The Korea National Health and Nutritional Examination Survey (KNHANES) reported that 3% of the population ≥30 years old experience stroke. Concerning CAD, the prevalence rate of <1% in 1998 has increased up to 2.5% in 2010.7) I t is d ifficult to note changes in the incidence rate of CVD owing to the lack of a nation-wide continuous monitoring system, however, recent research estimated that the annual incidence rate of acute myocardial infarction (AMI) was about 50 cases per 100000 males and about 20 cases per 100000 females.8) The incidence rate of cerebrovascular diseases depends on the type (i.e., cerebral infarction or cerebral hemorrhage), such that the incidence rate of cerebral hemorrhage is expected to decline rapidly, whereas that of cerebral infarction is expected to gradually increase. Therefore, the number of patients with cerebral infarction is expected to be greater than the number of patients with cerebral hemorrhage. The difference in the incidence of CVD according to the geographic region and year is predominantly explained by the change in the distribution of cardiovascular risk factors. The prevalences of diabetes and dyslipidemia are increasing, whereas there has not been much change in the prevalence of hypertension and the rate of smoking cessation in Korea. Therefore, CAD is expected to be the most prevalent type of CVD in Korea.
2. Risk factors and risk evaluation of cardiovascular disease in Korea
Knowing a person's cardiovascular risk factors is very important in terms of both prevention and management; however, each method of risk factor evaluation is different depending on the country-specific treatment guidelines. In 2009, the presence of a history of existing CAD or its equivalent risk factors, including carotid artery disease, peripheral artery disease (PAD), abdominal aneurysm, and diabetes, was defined as high risk, according to the revised Korean Guidelines for the Management of Dyslipidemia. Moreover, according to the revised National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) guidelines of treatment in 2004, risks were scored on the basis of the number of cardiovascular risk factors such as nonsmoking rate, hypertension, low high-density lipoprotein (HDL) cholesterol, age, and family history of premature CAD. Persons with two or more risk factors were classified as the intermediate risk group, whereas those with none or only one risk factor were classified as the low-risk group.9)
From 1996 through to 2004 in Korea, the Korean Heart Study, on 430920 male and female subjects who participated in nationwide health check-ups in 18 health promotion centers, was conducted. In this study, the observation of the incidence and risk factors for cerebrovascular diseases was followed for 10 years. The study results showed that the most influential risk factors on cerebrovascular diseases were hypertension, nonsmoking status, and dyslipidemia in male patients, and hypertension, dyslipidemia, diabetes, and nonsmoking status in female patients.5) In addition, the relative risk, which describes the risk of incident CVD or cerebrovascular diseases, of each risk factor was analyzed. The results showed that the association of smoking and dyslipidemia with CAD was stronger than that with cerebrovascular diseases, whereas the association of hypertension with cerebrovascular diseases was greater than that with CADs. Total cholesterol levels ≥200 mg/dL increased the risk of CAD, compared with levels <200 mg/dL, and increased the levels of HDL cholesterol, resulting in the risk of both CVD and cerebrovascular diseases. Overall, the Korean-specific risk factors for CVD included hypertension, smoking, dyslipidemia, and diabetes, all of which are similar to those from other countries, and a Korea-specific, 10-year CAD risk-scoring system based on these established risk factors is also currently available. However, validation of this scoring system and the indication for lipid-lowering medications according to the scored risks, as well as further study are needed to provide appropriate treatments for the Korean population.
3. Distribution of serum lipid profile in Koreans
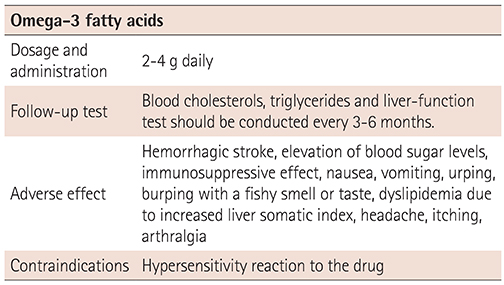
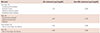
The average serum levels of total cholesterol in Korean male adults (age, ≥20 years) were 183 mg/dL in 2005, 188 mg/dL in 2010–2012, 183 mg/dL in 2005, and 189 mg/dL between 2010 and 2012. The levels have been increasing by about 5–6 mg/dL for the last 7 years between 2005 and 2012.
By contrast, between 2010 and 2012, the average triglyceride levels were 153 mg/dL in males and 112 mg/dL in females, exhibiting much less variability compared with the total cholesterol levels. During this period, the serum levels of low-density lipoprotein (LDL) cholesterol averaged 112 mg/dL in males and 115 mg/dL in females, whereas the levels of HDL cholesterol averaged 47 mg/dL in males and 52 mg/dL in females, thereby making the increment approximately 1 mg/dL for both LDL and HDL cholesterol levels, compared with the period between 2007 and 2009 (Table 1-1).1)
For adults older than 30 years, the prevalence of hypercholesterolemia (2010–2012) was 12.6% in males and 14.9% in females, which increased by 5.4% in males and by 6.5% in females during a 7-year period since 2005. By age group, the prevalence rate was highest in males in their 50s and females in their 60s (16.9% and 32.2%, respectively).
The prevalence rates of hypertriglyceridemia, defined by a total cholesterol level of ≥240 mg/dL or taking lipid-lowering agents (2010–2012), were 22.9% in males and 10.4% in females, with no significance difference from those in 2005. However, when specified by sex, the prevalence rate was two-fold higher in males than in females. By age, the highest prevalence rates were observed in males in their 50s (28.3%) and females in their 60s (17.5%).1)
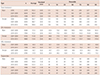
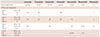
From 2010 through to 2012, the awareness rate of hypercholesterolemia was 45.2% in males and 49.1% in females, whereas the treatment rate was 35.8% in males and 38.4% in females, both of which increased by approximately 20% compared with those in 2005. The proportion of controlled hypercholesterolemia was about 30%, whereas that of treated patients was approximately 80%, which increased by ≥15% compared with that in 2005. In comparison by sex, the awareness and treatment rates of female patients were slightly higher than those of male patients. By age group, the awareness rate and treatment rate in subjects in their 30s–40s were 25% and 15%, respectively, which were much lower than those in the other age groups (Table 1-2).1)
Chapter 2. Criteria for the Diagnosis and Treatment of Dyslipidemia
1. Evaluation of laboratory lipid and diagnostic criteria
For the screening of dyslipidemia in persons ≥20 years old, testing of fasting serum lipid levels (total cholesterol, triglycerides, HDL cholesterol, and LDL cholesterol) is recommended every 4–6 years.10)
To acquire the triglyceride and LDL cholesterol levels among the lipid profiles, fasting for at least 9–12 h before venous sampling is required. The subject should be relaxed in the sitting position for at least 5 min before venous sampling, to avoid hemoconcentration due to excessive movement. Collecting tubes without an anticoagulant is recommended for serum samples, and EDTA tubes are recommended for plasma samples. When plasma samples are used for analyses, the results are generally lower by approximately 3% than those for serum samples.11)
Generally, the LDL cholesterol levels can be mathematically estimated, by using the fasting levels of total cholesterol, triglycerides and HDL cholesterol. If the triglyceride level is ≤400 mg/dL, it can be divided by 5 to estimate the level of very low density lipoprotein (VLDL) cholesterol. As the total cholesterol is the sum of LDL cholesterol, HDL cholesterol, and VLDL cholesterol, the value of LDL cholesterol concentration can be calculated according to the following Friedewald formula:
However, if a subject has a triglyceride level of >400 mg/dL, the mathematically estimated level of LDL cholesterol with the formula suggested above will be significantly lower than its actual value. Therefore, in this case, direct assay of LDL cholesterol levels can be used. In addition, direct assay of LDL cholesterol should also be used in subjects who had not fasted for at least 9 h.
A recent study, however, reported that the value of LDL cholesterol concentration calculated by using the Friedewald formula is significantly lower than the results obtained from direct assays,12) and this discrepancy should be accounted for in the diagnosis and treatment of dyslipidemia. Therefore, clinicians should ensure to use the same method to evaluate and longitudinally monitor the LDL cholesterol levels. In addition, because variabilities in the accuracy of test results among different manufacturers have been observed, this should also be accounted for when diagnosing dyslipidemia.13)
To establish the guidelines for the treatment of dyslipidemia, lipid levels should be tested at least twice, at different time points. If there is a significant difference between the results from the first and second tests, then a third test should be conducted to decide the treatment goals according to the finally verified lipid level.11)
The criteria for the diagnosis of dyslipidemia according to KNHANES are shown in Table 2-1.
The US NCEP criteria for lipid and lipoprotein levels can be used to evaluate the performance of a clinical laboratory for testing of the blood lipid level that is required for the diagnosis and treatment of dyslipidemia.14)
2. Treatment target
1) Introduction
The ACC/AHA guidelines on the treatment of blood cholesterol were published in 2013, after the revised ATP III guidelines were announced in 2004.4) Without the criteria for LDL cholesterol goal, the 2013 ACC/AHA guidelines recommended to administer high-intensity statins (expected to lower LDL cholesterol concentration by ≥50%) or moderate-intensity statins (expected to lower LDL cholesterol concentration by about 30–50%), depending on the risk levels. However, the degree of decrement in lipid levels per administration intensity greatly varies among patients, and thus, administering moderate-or high-intensity statins to all patients without certain therapeutic goals does not seem to be supported by sufficient evidence. Considering the fact that the results from Asian studies were not included in the establishment of the 2013 ACC/AHA guidelines, a study on the benefits and adverse effects of high-intensity administration in Asia, including Korea, is necessary. In addition, the 2013 ACC/AHA guidelines recommend the administration of statins for primary prevention in patients with a 10-year risk of atherosclerotic CVD (ASCVD) of ≥7.5%. However, this recommendation has been reported to overestimate the risk of ASCVD in Europeans and Asians,15)16) thereby making it not generally applicable to Asians. This has aroused the need for the establishment of new criteria generally applicable to the Korean population. However, owing to the insufficient data on cardiovascular risk from large-scale Korean cohort studies, the criteria should be established on the basis of currently existing Korean and international guidelines, and further be validated.
2) New Korean criteria for treatment
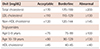
New Korean treatment guidelines, as in the previous Korean guidelines of treatment, determines the presence of cardiovascular risk factors and maintains the same structure, in which the goal of LDL cholesterol concentration is graded according to the risk level. However, they were further modified and revised according to Korean and foreign research results, as well as 2013 ACC/AHA guidelines (Table 2-2, 2-3, and 2-4).
(1) Very high risk
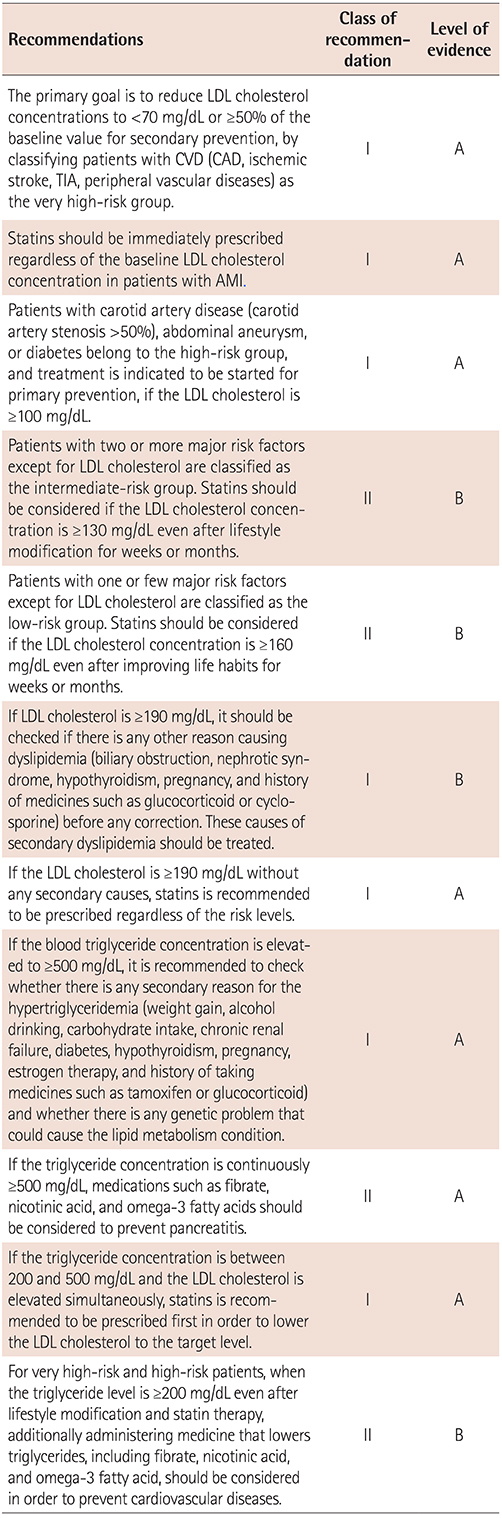
Patients with CVD (CAD, ischemic stroke, transient ischemic attack [TIA], or PAD) are classified as very high risk, and targeting LDL cholesterol <70 mg/dL or reducing ≥50% of the baseline value is indicated for secondary prevention (class of recommendation I, level of evidence A).
This recommendation is based on the results from multiple studies with subjects with a recent history of angina,17) ischemic stroke, TIA,18) and peripheral vascular diseases,19) in which the maximal preventive effect against CVD was seen when the level of LDL cholesterol was lowered to <70 mg/dL or <50% of the baseline levels with statin therapy. However, there is a need to conduct a nationwide study in the future, in order to establish the Korean-specific goal of LDL cholesterol levels. In consideration of previous Korean and global research results,20)21) immediate statin therapy is recommended to be started in patients with AMI, regardless of the baseline LDL cholesterol concentration (I, A).
(2) High risk
Although classified as high risk in the previous guideline, patients with a history of CVD are separately classified as very high risk in the revised version of the guideline. Meanwhile, patients with carotid artery disease (carotid artery stenosis >50%), abdominal aneurysm, or diabetes, which are risk factors equivalent to CAD, are classified as having a high risk, as in the previous treatment guidelines. Therefore, treatment is recommended to be started for primary prevention if the LDL cholesterol level is ≥100 mg/dL (I, A). Some previous studies reported that carotid artery diseases result in the increased risk for CVD,22) whereas studies on patients without CVD but with carotid artery stenosis reported that the decrease in LDL cholesterol levels after statin therapy helped reduce major cardiovascular events and mortality rates.23) Likewise, the presence of an abdominal aortic aneurysm increases the cardiovascular mortality by approximately 1.9%, even without accompanying CVD,24) and the administration of statins resulted in a significant improvement in the size of the aortic aneurysm and postoperative mortality in both the short term and the long term.25)26)27) In addition, administration of statins in subjects with type 1 and type 2 diabetes decreased the all-cause mortality and major cardiovascular risks.28)29)30) Therefore, stains may be required for such high-risk patients.
(3) Intermediate risk
The classification of the intermediate-risk group in the new guidelines follows the previous Korean treatment guidelines, in which moderate risk is defined as the presence of two or more major risk factors (Table 2-4), except for the LDL cholesterol criteria. Likewise, starting statin therapy should be considered in patients with LDL cholesterol levels ≥130 mg/dL even after appropriate lifestyle modification for weeks and months (II, B). Each component constituting major risk factors is established according to the preexisting ATP-III guidelines and current Korean guidelines. Previous studies showed that a nonsmoking status, hypertension, low HDL cholesterol, and a family history of CVDs are associated with increased incidence of CVD.31)32)33)34) Moreover, it was reported that increasing age leads to increased cardiovascular risk; however, females show similar risks of CVD to those of males after 10–15 years.35) However, it was reported that such major risk factors can predict only half of the actual risk of CVD.11) Therefore, other risk factors such as obesity, physical activity, dietary habits, triglycerides, high-sensitivity C-reactive protein, lipoprotein (a), apolipoprotein, fibrinogen, homocysteine, apolipoprotein B, anklebrachial blood pressure index, carotid intima-media thickness (clinically suspected progression even with <50% stenosis or the presence of atherosclerotic plaques), and coronary calcium score should be considered to establish an individualized therapeutic goal.11)
(4) Low risk
Patients with one or few major risk factors (Table 2-4), except for LDL cholesterol, are classified in the low-risk category. For this group, it is reasonable to start statins, as in the previous treatment guidelines, if the LDL cholesterol concentration is ≥160 mg/dL even after modifying lifestyle for weeks or months (II, B).
Although the revised guidelines defined the LDL cholesterol goal as <160 mg/dL as in the previous treatment guidelines, a more intensified treatment goal also is reasonable for low-risk patients depending on the case, as other risk factors can be considered other than the major risk factors in the intermediate-risk group, as mentioned above (II, B).11)
In particular, if LDL cholesterol is ≥190 mg/dL, it is necessary to check if there are other causes of dyslipidemia (biliary obstruction, nephrotic syndrome, hypothyroidism, pregnancy, and history of taking medicines such as glucocorticoid and cyclosporine) before any treatment.4) If LDL cholesterol is found to be ≥190 mg/dL without any secondary causes, starting statin therapy is recommended regardless of risk levels, which also complies with the 2004 ATP III revision9) and the 2013 ACC/AHA treatment guidelines (I, A).4)
(5) Guidelines of treatment for hypertriglyceridemia
For the treatment guidelines for hypertriglyceridemia, if the blood triglyceride concentration is elevated to ≥500 mg/dL, it is recommended to determine if there is any secondary cause: weight gain, drinking, carbohydrate intake, chronic renal failure, diabetes, hypothyroidism, pregnancy, estrogen therapy, history of taking medicines such as tamoxifen or glucocorticoid, and/or genetic issues (I, A).4) In addition, if the blood triglyceride concentration is elevated to ≥500 mg/dL, it is known that there is a risk of acute pancreatitis.36) Therefore, if the triglyceride concentration is continuously found to be ≥500 mg/dL even after the above-mentioned causes have been corrected, starting medication with fibrate, nicotinic acid, or omega-3 fatty acid should be considered (II, A), which also complies with the ATP III11) and the ESC/EAS guidelines.3)
If the triglyceride concentration is between 200 and 500 mg/dL, it is recommended to prescribe statin therapy, as the first treatment, according to the calculated cardiovascular risk level (I, A).
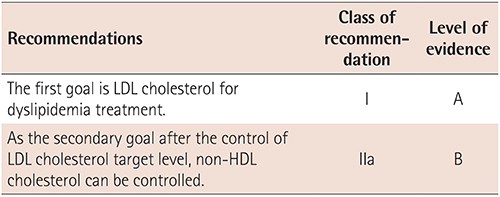
As the secondary goal, adjusting the non-HDL cholesterol level may be considered. As previously mentioned, the treatment goal should be adjusted according to the criteria in Table 2-3, by calculating the non-HDL cholesterol concentration (=Total cholesterol–HDL cholesterol) (II, B). The target concentration of non-HDL cholesterol can be acquired by adding 30 to the existing LDL cholesterol target. When the triglyceride (TG) level is ≥200 mg/dL in a patient with hypertriglyceridemia even after lifestyle modifications and statin therapy, it is reasonable to prescribe triglyceride lowering agents (e.g., fibrate, nicotinic acid and omega-3 fatty acid) in addition to statins for those patients that belong to a very high-risk or high-risk group in order to prevent CVD (II, B); however, there is a need for a future study on the usefulness of such combination therapy because it is still a controversial issue.37)
3) Conclusion
In conclusion, although there would be many issues in applying the 2013 ACC/AHA guidelines to Koreans, the goal of the revised treatment guidelines is to prevent delays in the treatment by separating the very high-risk patient group and stratifying the criteria, in consideration of the fact that statin should be started immediately for those with CVDs or with the equivalent risk factors. Still, there will be a need for an additional study on the domestic population, with respect to the statin dosage and LDL cholesterol goal appropriate to Korea as well as hypertriglyceridemia control goal for primary prevention.
3. Monitoring of lipids and enzymes
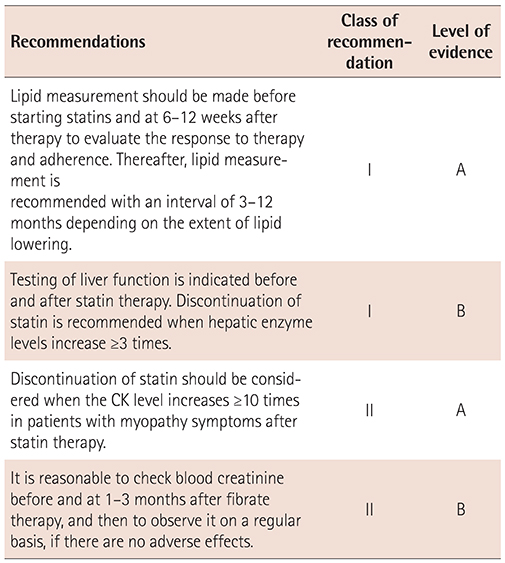
In the revised guidelines, the recommendation levels consider both the existing domestic guidelines and the global guidelines.3)4) It is recommended to evaluate the response to treatment and the patient compliance by conducting the lipid test before treatment, and to repeat the same test again in 6–12 weeks after starting medication, and then at intervals of 3–12 months depending on the degree of lipid lowering and the patient's cardiovascular risk level (I, A).
Liver function test should be conducted before the initiation of statin therapy, and then the follow-up test should be conducted together with the lipid test after statin therapy. It is indicated that statin should be discontinued when the hepatic enzyme levels are elevated to ≥3 times the normal levels (I, A). In addition, if a patient complains of muscular pain and weakness, and if creatine kinase (CK) is ≥10 times the normal level after taking statins, it is reasonable to stop the administration owing to the diagnosis of myopathy (II, A).
In addition, as previous studies reported slight elevation of blood creatinine after fibrate therapy, the domestic guidelines also suggest checking the creatinine level before and after 1–3 months of fibrate therapy. If there is no further abnormal findings afterwards, it is reasonable to perform follow-up on a regular basis (II, B).3)
Chapter 3. Lifestyle Modifications for Dyslipidemia
In the prevention and treatment of dyslipidemia, lifestyle modifications are very important. To lower the risk levels of dyslipidemia, cessation of smoking is very important, whereas improvement of eating and exercise habits is also important in order to reduce the risk levels of dyslipidemia and for treatment purposes.
1. Diet
1) Energy
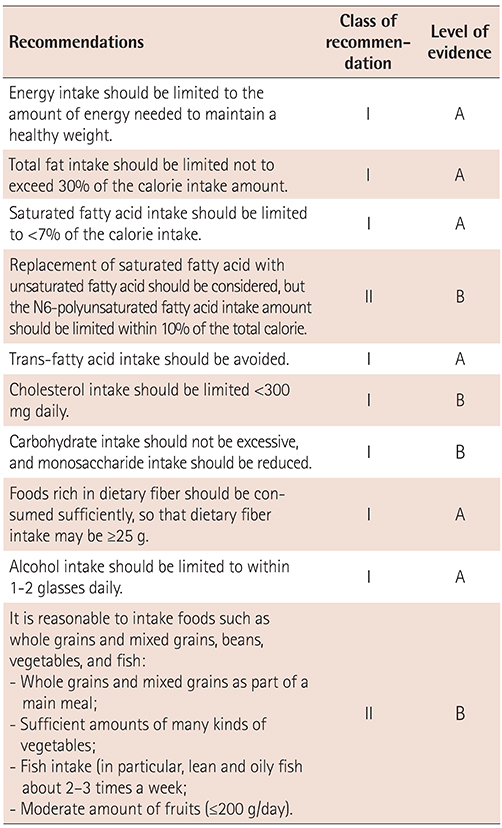
Obesity and weight gain are associated with the onset of dyslipidemia. Many studies with obese or overweight subjects have reported that the levels of total cholesterol, LDL cholesterol, and triglycerides in blood decreased after weight reduction.38) Therefore, maintaining weight at the approximate level requires controlling the energy intake.3)4) Generally, a body mass index (BMI) of ≥30 kg/m2 is classified as obesity. However, there is an opinion in Korea that any BMI ≥25 kg/m2 should be classified as obesity. Patients with obesity can improve their cholesterol and triglyceride levels by losing weight by about 5–10%, despite failing to achieve a normal body weight. It is generally known that a low-calorie diet with an energy intake reduced by about 500 kcal than normal causes no special harm to a person's health and is easy to follow.
2) Fat
It has been traditionally recommended to limit fat intake for dyslipidemia treatment. Indeed, some reports showed that reduced fat intake improves blood LDL cholesterol level; however, in most cases these are compound reduction effects of losing weight, both for reduced saturated fat and trans fat intake. In addition, it is difficult to determine the effect of reducing the total fat intake. Moreover, fat limitation relatively increases carbohydrate intake, and it is found that increasing carbohydrate intake elevates the blood triglyceride level.39) However, a high fat intake may have a negative impact on blood lipid levels by increasing the intake of saturated fat and energy, and thus fat intake should be maintained at an appropriate level.
The ESC/EAS guidelines recommended not to increase fat intake in excess of 35% of the total calories.3) The fat intake in Koreans is about 20% of the total calorie intake. The Dietary Reference Intake for Koreans recommends that the appropriate fat intake should be 15–25% of the total calories. Fat intake in Korea is lower than that in Western countries40); however, there is a wide variation depending on each person, with increasing fat intake in recent years. It is well known that the types of lipid have more impact on blood lipid levels rather than the amount of total fat intake, and it is necessary to ensure that fat intake does not exceed 30%.
Rather than limiting the amount of total fat intake, the influence of the type of fatty acids on the blood lipid levels should be taken into account. It was found that if saturated fatty acids were replaced with unsaturated fatty acids, the level of blood LDL cholesterol can be lowered, and that there is a positive influence on the levels of blood triglycerides and HDL cholesterol if trans fatty acids were replaced with unsaturated fat.41) Therefore, for the treatment of dyslipidemia, there is a need to limit the intake of saturated fatty acids and trans fatty acids. The ATP III and ESC/EAS guidelines recommend limiting the intake of saturated fatty acids to <7% of the total energy,3)11) whereas the ATP III and 2013 ACC/AHA guidelines recommend minimizing the intake of trans fatty acids.4)11) Saturated fatty acids are mainly found in meat fat, poultry skin, butter, and palm oil. The major sources of trans-fatty acids are hydrogenated oil, including margarine and shortening, and high amounts of trans fatty acids are also contained in oils treated for a long time at a high temperature.
Omega-3 fatty acids have no positive effect on blood cholesterol levels; however, hypertriglyceridemia can be lowered if 2–4 g is taken daily.42)
Replacement of saturated fatty acids with polyunsaturated fatty acids is effective in improving the blood cholesterol and triglyceride levels; however, it is recommended to take <10% of the total energy in order to prevent lipid peroxidation of plasma lipoprotein.
Cholesterol intake has less influence on the blood LDL cholesterol level, and there are wide individual variations in both saturated fat and trans fat. However, it is desirable to avoid excessive cholesterol intake. The ESC/EAS guidelines recommend an intake of <300 mg daily.3)
3) Carbohydrate
Excessive carbohydrate intake, especially excessive monosaccharide intake, increases the blood triglyceride level. Soluble dietary fiber is effective in improving blood cholesterol and triglyceride levels.43) Therefore, it is recommended to reduce monosaccharide intake and to consume mixed grains, marine algae, and vegetables that contain large amounts of soluble dietary fiber.
ATP III recommends 10–25 g of soluble dietary fiber daily, whereas the ESC/EAS guidelines recommend 5–15 g of soluble dietary fiber daily (25–40 g of the total dietary fiber).11)
Sufficient amount of food rich in dietary fiber should be taken so as to reach a fiber intake of ≥25 g.
4) Alcohol
Excessive alcohol intake (≥10–30 g/day) should be avoided because it affects the blood triglyceride level.44) Hypertriglyceridemia caused by alcohol intake is associated with decreased activity of lipoprotein lipase, which results in the inhibition of chylomicron catabolism. The ESC/EAS guidelines recommend that alcohol consumption should be limited to 1–2 glasses/day (males: <20–30 g, females: <10–20 g), and even to stop drinking especially in patients with hypertriglyceridemia.3)
5) Dietary pattern
More recently, there are many studies being conducted not on the respective nutrients but on the relations between diet pattern and diseases. Eating habits are classified according to the types food or their combination. In Western countries, there are studies currently being conducted on the effects of eating habits such as the Dietary Approaches to Stop Hypertension (DASH) diet and the Mediterranean diet on blood lipid levels. On the basis of such studies, the 2013 ACC/AHA guidelines recommend applying diet plans such as the DASH diet, US Department of Agriculture food pattern, and AHA diet.4) In Korea, there are only a few studies on the relationship between dyslipidemia and eating habits. However, it will be helpful to have a diet that includes a higher portion of whole grains such as mixed grains, brown rice, and whole wheat, with foods such as vegetable, beans, fish, fruit, and dairy products.45) On the basis of many previous studies, it is helpful to sufficiently consume fruit and vegetables, in order to prevent and treat dyslipidemia. However, carbohydrate accounts for a relatively higher portion of the Korean diet with fruit consumed as dessert and eating between meals rather than as a regular diet. Extra care should be paid because extra consumption of fruit may increase the monosaccharide intake. The ESC/EAS guidelines recommend taking about 200 g of fruits daily.3) Table 3-1 shows how to select foods appropriately.
< Examples of rough estimates per fruit type, equivalent to 200 g >
1 small apple, 2 tangerines, 1 orange, 1 small oriental melon, 1 tomato, 2 kiwis, or 1 persimmon
*1. Please use this only as reference because the actual size of the fruit may vary according to the subjective point of view.
2. Consider as medium size any fruit whose size is not indicated herein.
2. Exercise
1) Exercise and its effects on lipid metabolism
Whether or not regular exercise leads to any changes in blood lipid levels is controversial because various results have been reported depending not only on the subjects' sex, age, race, and lipid concentration but also on the type, amount, intensity, duration, and frequency of exercise, as well as on whether lifestyle and body weight changed with regular exercise habits.46) Moreover, regular exercise does not have a great impact on lipid levels. Exercise is classified as either aerobic exercise or anaerobic exercise. It was reported that there are some differences in the change of cholesterol level according to exercise types.
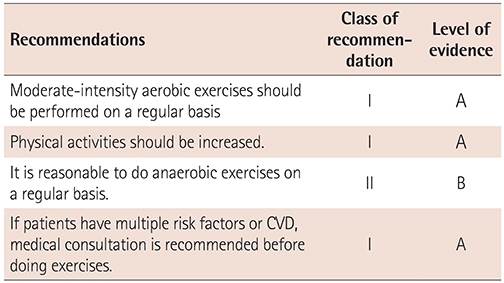
Aerobic exercises increase physical oxygen consumption; these exercises include walking at a rapid pace, jogging, swimming, and bicycling that can be maintained for ≥30 min, enhancing cardiovascular endurance. Meanwhile, anaerobic exercises include short-distance running, push-ups, throwing, and jumping within 10 s, which are good for strengthening muscles by using instant power.
In general, aerobic exercises help reduce triglycerides and increase HDL cholesterol level, with minor changes in LDL cholesterol.47)48) Exercise therapy undoubtedly prevents CVD; however, such effects are not very clearly observed. The goal of controlling lipid metabolism is to prevent CVD, and exercise therapy is important for a patient with dyslipidemia.46)49)
The effects of anaerobic exercises on lipids is more controversial.50)51) For other CVDs, their effect of controlling risk factors are lower than those of aerobic exercises. However, anaerobic exercises increase muscle mass and muscle strength, increasing physical activities and improving daily performance especially for older persons.46)
Healthy adults may start aerobic exercises with moderate or less intensity, whereas elderly persons or those with multiple risk factors or CVD need medical consultation before starting exercise, and are subjected to a cardiovascular stress test by using a treadmill or a bicycle, if needed.46) Medical assessment is required before a patient starts performing anaerobic exercises. Therefore, not only exercises but also increasing physical activities are recommended because these are both associated with the prevention of CVD.52)
2) Exercise prescription
There are no special exercise prescriptions for controlling dyslipidemia; however, the same methods are used to prevent CVD.46)53)
The types of recommended aerobic exercises include walking at a quick pace, jogging, swimming, or bicycling. The appropriate frequency is 4–6 days/week, whereas the intensity is 55–75% of the maximum heart rate (=220–age). However, the target heart rate should not be applied to a patient with CVD who is taking a β-blocker or nondihydropyridine calcium-channel blockers. When the intensity of the exercise starts to feel "moderate," it is good to intensify the exercise and maintain it at the level of "a little tough".
Warm-ups should start with light stretching and walking for 5–10 min, followed by 30–60 min of aerobic exercises as the main workout. It is possible not only to do continuous exercises but also to do them in 10-min sets. Then, complete it with some light walking and stretching for 5–10 min. Table 3-2 summarizes the exercise therapy for patients with dyslipidemia.
Chapter 4. Pharmacological Therapy for Dyslipidemia
1. Selection of drugs
It is important to combine lifestyle modification together with medication. Lifestyle modification includes diet therapy, exercise therapy, or abstaining from smoking. To determine whether to start drug therapy, a comprehensive consideration should be given to both the risk level of CVD and the LDL cholesterol levels. The risk level for CVD should be classified as one of the following: low, intermediate, high, or very high.
The treatment with drugs can be initiated according to whether the patients have CAD, PAD, ischemic cerebral infarction, atherosclerotic artery disease (aortic aneurysm, TIA, severe carotid artery stenosis), or diabetes, as well as on the number of CAD risk factors (smoking, hypertension, low HDL cholesterol level, family history of premature CAD, and age).
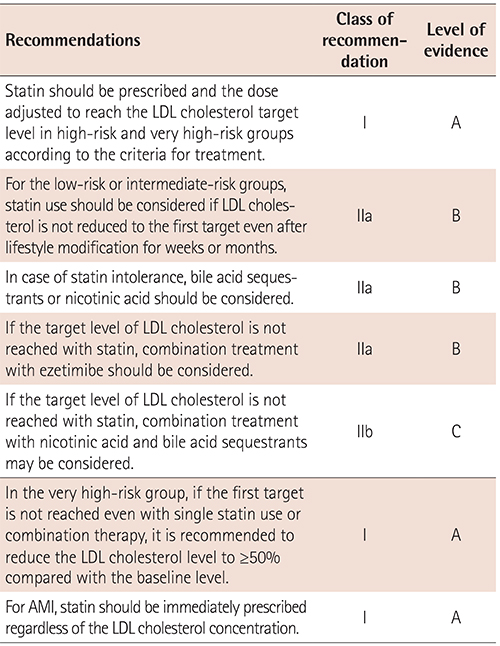
Statin is the first-choice drug for the treatment of hypercholesterolemia. The dosage is recommended to be adjusted to reach the target LDL cholesterol level according to the cardiovascular risk level (class of recommendation I, level of evidence A).3)4)
The first goal for drug therapy is to lower the LDL cholesterol to the target level or below (I, A), whereas the secondary goal is to lower the non-HDL cholesterol to target level or below (IIa, B).11)
Secondary causes of hypercholesterolemia should be considered and corrected before starting any medication (Table 4-1).
1) Low density lipoprotein cholesterol
Very high-risk group: This group includes patients with CAD, PAD, and/or ischemic stroke. The goal is to reduce LDL cholesterol concentration to <70 mg/dL or to reduce it by ≥50% than the baseline value (I, A). Statin treatment can be considered regardless of the baseline LDL cholesterol level.3)4) There are some reports on additional beneficial effects on clinical prognosis for patients with acute coronary syndrome (ACS), when LDL cholesterol is lowered down to 54 mg/dL.
For patients with AMI, statins is indicated to be administered immediately regardless of the baseline LDL cholesterol concentration (I, A).20)21)
High-risk group: This group includes patients with atherosclerotic artery disease (aortic aneurysm, TIA, or carotid artery stenosis >50%) or diabetes. If the LDL cholesterol is ≥100 mg/dL, statin medication should be started (I, A), and can be considered in selected patients whose LDL cholesterol level is <100 mg/dL.28)29)30)
Intermediate-risk group: This group includes patients with two or more cardiovascular risk factors (smoking, hypertension, low HDL cholesterol, and family history of premature CAD). Starting statin medication should be considered if the LDL cholesterol level is ≥130 mg/dL (IIa, B). It can also be initiated in patients with multiple risk factors when their LDL cholesterol level is 100–129 mg/dL.
Low-risk group: This group includes patients with one or few cardiovascular risk factors (smoking, hypertension, low HDL cholesterol, and family history of premature CAD). If the LDL cholesterol level is ≥160 mg/dL, statin medication should be considered (IIa, B).
2) Triglycerides
If the triglyceride concentration is high, it is recommended to first determine whether there are other factors increasing triglycerides and then to establish the treatment plan by evaluating the cardiovascular risk level (Table 4-1).
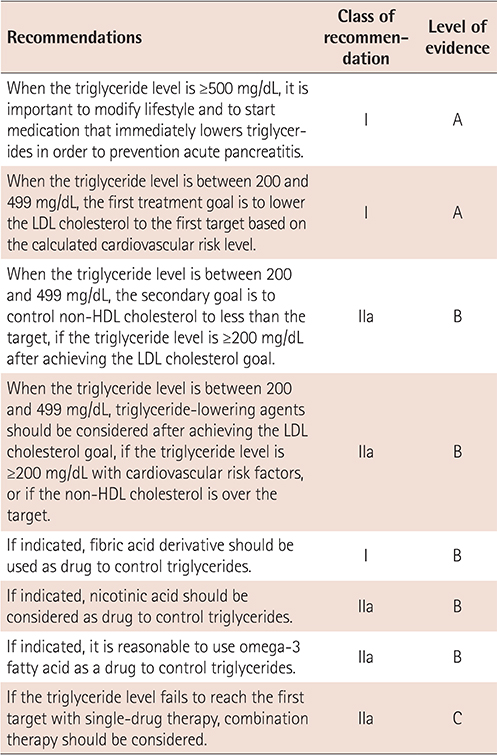
As about 10% of acute pancreatitis is known to be caused by hypertriglyceridemia, it is important to modify lifestyle and medication should be started immediately to prevention acute pancreatitis, when the triglyceride concentration is ≥500 mg/dL (I, A). Lifestyle modification with a low-fat diet (reduced to 10–15% of the caloric intake) and cessation of drinking are required. Combined with lifestyle modification, medication should be started first by using fibric acid derivatives (I, B), nicotinic acid (IIa, B), or omega-3 fatty acids (IIa, B), which mainly lower triglycerides. For a diabetic patient, it will be helpful to strictly control blood glucose by using insulin, whereas apheresis can be helpful if there is a need to achieve rapid reduction.54)
When the triglyceride level is between 200 and 499 mg/dL, the first treatment goal is to lower the LDL cholesterol to the target level based on the calculated cardiovascular risk level (I, A). Therapeutic lifestyle modification and statin medication can be considered to achieve the goal. After achieving the LDL cholesterol goal, when triglycerides are still ≥200 mg/dL, it is reasonable to use triglyceride-lowering agents especially for the high-risk and very high-risk groups (IIa, B). Fibric acid derivatives (I, B), nicotinic acid (IIa, B), and omega-3 fatty acids (IIa, B) are used to control triglycerides.55)56)57) When the triglyceride level fails to reach the target level with a single agent, combination therapy should also be considered (IIa, C).
2. Characteristics of lipid-lowering agents
1) Statins: 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors
Statins are first recommended for the treatment of dyslipidemia among currently available drugs because it has a relatively low risk profile and proven effects of decreasing CVD by lowering LDL cholesterol.58)
(1) Action mechanism
All types of statins reduce cholesterol synthesis by competitively inhibiting 3-hydroxy-3-methylglutaryl coenzyme A reductase, which is a cholesterol precursor.59) In hypercholesterolemia, to maintain homeostasis in the cellular level, the expression of LDL receptors should increase and the synthesis of cholesteryl ester should decrease.
As a result, more blood LDL cholesterol is removed and production of VLDL cholesterol decreases in the liver, resulting in the decrease of LDL cholesterol. Statins not only block such synthesis but also inhibit the synthesis of lipid intermediates, which have important biological effects. Metabolites such as geranylgeranyl pyrophosphate and farnesyl pyrophosphate prenylate proteins. Through this process, the molecules are attached to the cell membrane, enhancing their biological activities. The geranylgeranylation of Rho A and the inhibition of phosphorylation of peroxisome proliferator-activated receptor alpha, which regulates the transcription of apo A1, are considered as the mechanisms of how statin raises the HDL cholesterol level. Alteration of protein prenylation seems to mediate some effects of statins other than their LDL cholesterol-lowering effect.
(2) Types of statin
The currently available statins include lovastatin, pravastatin, simvastatin, fluvastatin, atorvastatin, rosuvastatin and pitavastatin.
(3) Effects on lipid level
Each statin is different in terms of absorption, blood protein binding, excretion, and solubility, with variable LDL cholesterol-lowering effects per dosage (Table 4-2).60)61)62)63)) When the statin dosage is doubled, the LDL cholesterol level additionally decreases by 6% in general. In addition, when statins are used in patients with hypertriglyceridemia, the triglyceride level also decreases by 22–45% because the VLDL cholesterol secretion in the liver is inhibited. HDL cholesterol slightly decreases by 5–10%. Many studies on Koreans have been reported concerning the lipid-lowering effect of each statin. Some domestic studies reported the tendency of higher LDL cholesterol-lowering effects with the same dosage in Koreans compared with Western people (Table 4-3, Fig. 4-1).64)
(4) Cardiovascular diseases prevention research and indications
①Secondary prevention effect of cardiovascular disease: It is widely known that patients with CVD (angina, ACS, AMI, stroke, or TIA) have increasing risks of cardiovascular events or death.17)18)19) For such patients, it is recommended to use statins because these drugs prevent the recurrence of cardiovascular events (I, A). The goal for these patients, classified as the very high-risk group, is to reduce LDL cholesterol to <70 mg/dL or ≥50% of the baseline level for secondary prevention.
In case of AMI, statins are indicated to be prescribed immediately regardless of the baseline LDL cholesterol level (I, A).20)21)
Although there are not many large-scale studies in Asians,65) there is a report on better preventive outcomes in patients ≤75 years old with CVD when they took statins to reduce LDL cholesterol by ≥30–50% from baseline levels. Therefore, it is reasonable to use moderate-dose/moderate-intensity or high-dose/high-intensity statin that can reduce the LDL cholesterol level by ≥30–50% from the baseline levels (IIa, A).
For patients aged >75 years with cardiovascular diseases, it is reasonable to start statin after considering comorbidities and possible drug-drug interactions (IIa, B).66)
②Primary prevention of cardiovascular disease in the general population: Adults with a blood LDL cholesterol level of ≥190 mg/dL have an increased possibility of having CVD during their lifetime. Therefore, statins should be prescribed if the blood LDL cholesterol concentration is ≥190 mg/dL even after lifestyle modification (I, A).3)4)
For an adult with a blood LDL cholesterol level of 160–190 mg/dL, it is reasonable to use statin if the blood LDL cholesterol is ≥160 mg/dL even after lifestyle modification for 4–8 weeks (IIa, B).
Meanwhile, for an adult with a blood LDL cholesterol of 130–160 mg/dL, lifestyle should be properly modified, and then it may be decided whether to start statins in consideration of cardiovascular risk level (IIb, C).
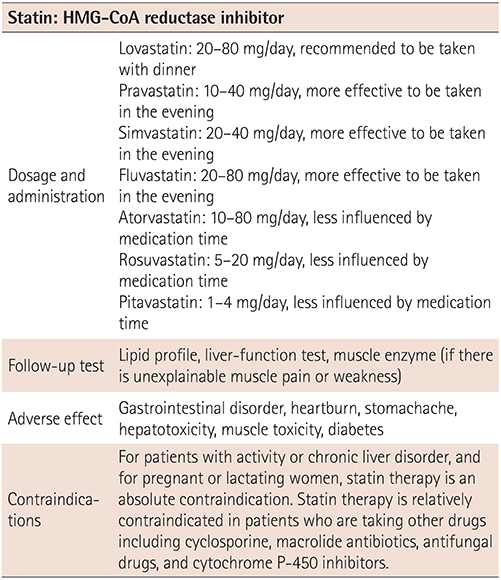
(5) Dosage and administration
Lovastatin: 20–80 mg/day, recommended to be administered with dinner
Pravastatin: 10–40 mg/day, more effective to be administered in the evening
Simvastatin: 20–40 mg/day, more effective to be administered in the evening
Fluvastatin: 20–80 mg/day, more effective to be administered in the evening
Atorvastatin: 10–80 mg/day, less influenced by the time of medication
Rosuvastatin: 5–20 mg/day, less influenced by the time of medication
Pitavastatin: 1–4 mg/day, less influenced by the time of medication
Pitavastatin: 1–4 mg/day, less influenced by the time of medication
(6) Follow-up test before/after statin medication
①Blood test before statin treatment: Before starting any statin treatment, the transaminase (aspartate transaminase [AST] and alanine transaminase [ALT]) concentrations should be measured (I, B). If the ALT concentration is ≥3 times than the normal range before medication, it is reasonable to first evaluate and treat liver diseases instead of immediately starting statins, and then to proceed with the statin medication after the liver function has normalized (IIa, C). If the baseline muscle enzyme (CK) is ≥3 times than the normal range, it is reasonable to identify the causes before starting any statin (IIa, C).
②Follow-up test after statin treatment: After the initiation of statin treatment, the cholesterol, triglyceride, and HDL cholesterol levels should be evaluated after 4–12 weeks (I, B). If LDL cholesterol is ≤40 mg/dL after two consecutive measurements, the statin dose may be reduced (IIb, C). Evaluation of liver function should be considered at 4–12 weeks after treatment. Thereafter, it is reasonable to repeat the test every 3–12 months to check the efficacy and hepatotoxicity of statins (IIa, C). Regular tests for muscle enzyme are not indicated (III, A).
(7) Adverse effect
The most common adverse effects that occur in about 4% of statin-treated patients include gastrointestinal disorder, heartburn, and stomachache; moreover, rare and fatal adverse events such as hepatotoxicity and muscle toxicity can also occur.58) In patients >75 years old, as well as in patients who are taking multiple drugs or taking drugs with same metabolic pathway as statins, or those with conditions that require complex medication (e.g., heart transplant or AIDS), statin should be considered in low dosage (IIa, C).
①Hepatotoxicity: If there is a slight increase in transaminase, there is no need to stop statin. Statins should be stopped when liver enzymes are elevated by ≥3 times the normal range. Restarting statins may be considered from a low dose after the normalization of liver enzymes (IIb, C). If there are any symptoms suggesting liver damage, such as fatigue, appetite decrease, stomachache, dark-colored urine, and jaundice, during statin treatment, it should be considered to immediately perform a liver function test including AST/ALT measurement (IIa, C).
②Muscle toxicity: The most common adverse effect during statin medication is muscle pain. About 10% of patients taking statins are reported to have muscle pain and, consequently, to stop taking statins. Many patients discontinue statin use because of muscle pain or weakness. However, it is not clear whether these symptoms are caused by statins. The frequency of muscle damage due to statin is known to be higher by 0.01% in patients who are taking statins than that in a control group.
The elevation of muscle enzyme due to muscle damage, resulting in rhabdomyolysis, hemoglobinuria, and acute renal failure, is known to occur in only a very small portion of patients. Muscle damage after statin treatment occurs more often in patients with multiple comorbid diseases or those with the concomitant use of cyclosporine, fibrate derivatives, macrolide antibiotics, or several antifungal drugs. Taking fibrate derivatives such as gemfibrozil with statin increases the risk of muscle damage, whereas fenofibrate is known to have a relatively low risk. The measurement of muscle enzyme in asymptomatic patients on a regular basis is not recommended (III, A). However, if there is muscle pain, weakness, or general fatigue, it is reasonable to measure the muscle enzymes to check if there is any muscle damage (IIa, C).
③Diabetes: Recently, some studies reported that statins increase the incidence of diabetes.70) In most cases, new-onset diabetes was diagnosed in persons with glucose intolerance before taking statins or in those who are taking high-dose statins. Therefore, measurement of the fasting blood glucose before taking statins is recommended (I, B). Even when diabetes occurs after statin use, it is recommended to continue taking statins in order to prevent CVD, in addition to lifestyle modifications such as regular exercise, weight control, and smoking cessation (I, B).
2) Fibric acid derivatives
(1) Indications
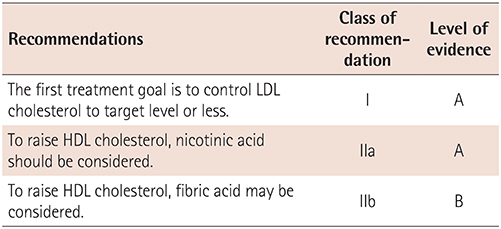
Fibric acid derivatives are recommended in patients with hypertriglyceridemia (I, B), and reasonable to combine with statins in patients with mixed dyslipidemia in whom both LDL cholesterol and triglycerides are increased (IIa, A).73)74) In addition, there are a number evidences showing that fibric acid derivatives reduce cardiovascular risk if prescribed to patients with high triglycerides and with low HDL cholesterol. However, it is not recommended as the first-line treatment in case of only a high LDL cholesterol level.
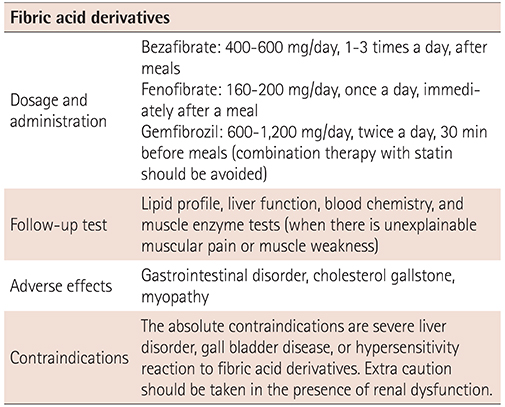
(2) Dosage and administration
Bezafibrate: 400–600 mg/day, 1–3 times a day, after meals
Fenofibrate: 160–200 mg/day, once a day, immediately after a meal
Gemfibrozil: 600–1200 mg/day, twice a day, 30 min before meals
(4) Adverse effect
The most common adverse effect is gastrointestinal disorder, and there may be increases in the prevalence of cholesterol gallstones. Myopathy may occur, but with a low frequency. If renal function is impaired, blood drug concentration increases, with higher risks of adverse events. In particular, when gemfibrozil is prescribed together with statins, the risk of myopathy increases, whereas fenofibrate is preferred in combination with statins owing to the low risk of myopathy. Fibric acid derivatives bind with albumin, thereby increasing the blood level of warfarin, with subsequent increase in bleeding tendency; moreover, fibric acid derivatives may increase the effect of hypoglycemic agents. Fibric acid derivatives increase blood creatinine concentration but do not cause renal failure.
3) Nicotinic acid (niacin)
(1) Indications
Niacin can be used for all types of dyslipidemia. For hypertriglyceridemia, it should be considered as the first-line medication (IIa, B), whereas nicotinic acid is effective for patients with low HDL cholesterol (IIa, A).76) For patients with high LDL cholesterol or mixed-type dyslipidemia, it may be considered to use nicotinic acid in combination with statins, if not treated with statin therapy alone; however, care should be taken because of the risk of increasing the adverse effects, including liver function disorder, myopathy, and increasing the incidence of diabetes (IIb, A).
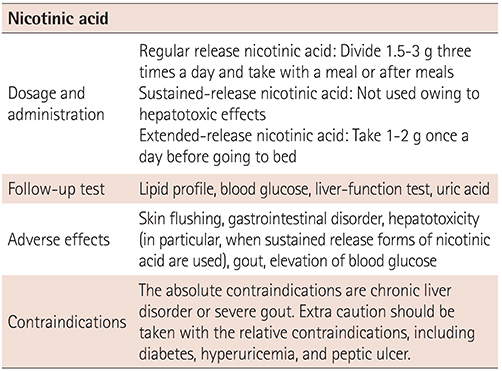
(2) Dosage and administration
Regular-release nicotinic acid: Divide 1.5–3 g into three times a day and take with a meal or after meals
Sustained-release nicotinic acid: Not used owing to hepatotoxic effects
Extended-release nicotinic acid: Take 1–2 g once a day before going to bed
(4) Adverse effects
Skin flushing is a common adverse effect, which can be very severe in some patients. Skin flushing could be reduced with long-term continuation of medication, and the adverse effects could be reduced with the administration of the drug with a meal or by taking aspirin. Gastrointestinal disorder is frequently observed. Other important adverse effects include hepatotoxicity, gout, and elevation of blood glucose levels, in proportion with dosage and the duration of therapy. The risk of hepatotoxicity increases with sustained-release nicotinic acid, and cases of fulminant hepatic failure have been reported. The frequency of facial flushing is known to be reduced with the use of recently developed drugs.
4) Ezetimibe
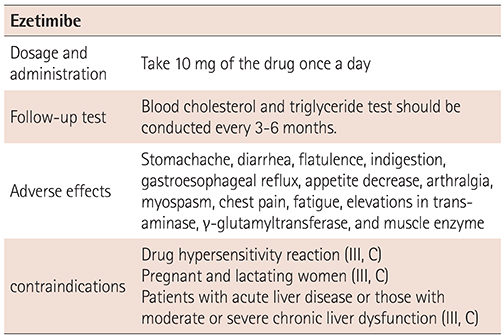
(4) Adverse effects
The common adverse effects include stomachache, diarrhea, flatulence, and gastrointestinal symptoms, whereas the relatively uncommon adverse effects include indigestion, gastroesophageal reflux, appetite decrease, arthralgia, muscle spasm, and chest pain. Increases in transaminase, γ-glutamyltransferase, and muscle enzymes have been reported.
(5) Contraindications
This drug is not recommended if there is a hypersensitivity reaction (III, C). For pregnant and lactating women, it is not recommended to use this drug owing to safety issues (III, C). It is also not indicated for use in patients with acute liver disease or those with moderate or severe chronic liver dysfunction (III, C).
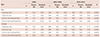
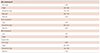
5) Omega-3 fatty acids
(3) Follow-up test
Blood lipid profile and liver-function test should be conducted at every 3–6 months.
(4) Adverse effects
Some of the reported adverse effects include hemorrhagic stroke, elevation of blood sugar levels, immunosuppressive effect, and dyslipidemia. Moreover, there are reports on gastrointestinal symptoms such as nausea, vomiting, burping, and burping with a fishy smell or taste, as well as on liver enzyme elevation, headache, itching, or arthralgia.
(5) Contraindications
There are no absolute contraindications for this drug, except for a hypersensitivity reaction. This drug belongs to pregnancy category C, and omega-3 fatty acids should be considered only if there are great benefits of using the drug (II, C). An animal study reported on fatal outcomes with excessive administration. There are no well-established safety issues yet concerning use on humans during pregnancy. It is also not known if this drug is secreted in breast milk.
Chapter 5. Dyslipidemia in Different Clinical Settings
1. Stroke (cerebrovascular diseases)
Dyslipidemia is one of the important risk factors of CVD; however, there is no clear association between dyslipidemia and stroke in general. Although stroke considerably contributes to the pathological mechanism of CVD, the association with dyslipidemia is not clear because of the various subtypes of cerebrovascular disease. Many cohort studies reported that low cholesterol levels are associated with the incidence and mortality rate of cerebral hemorrhage. Therefore, a more careful approach is needed in Korea, where the incidence and mortality rate of cerebral hemorrhage is relatively higher than those in Western countries. However, dyslipidemia is an important risk factor in cerebral infarction, especially in atherosclerotic cerebral infarction, and many clinical studies revealed that the risk of stroke could be decreased through statin therapy.
1) Primary prevention
Statin therapy in adults with CVD or in those with a high risk for CVD is effective for the primary prevention of cerebral infarction.80) The effects of other lipid-lowering agents on the primary prevention of stroke are still uncertain.
2) Secondary prevention
Stroke patients have increased risk not only of recurrent stroke events but also of the development of CVDs such as myocardial infarction. The subtype of stroke plays an important role in statin therapy for the secondary prevention of stroke. Statin therapy is the most effective treatment for atherosclerotic cerebral infarction; however it might be harmful in those with cerebral hemorrhage.
If there are CVDs or equivalent risk factors (carotid artery disease, PAD, abdominal aneurysm, diabetes, etc.), statins should be used for the primary prevention of stroke. The LDL cholesterol target level can be determined according to general recommendations.
High-intensity statin therapy is recommended to prevent the recurrence of stroke in patients with atherosclerotic cerebral infarction or TIA and in those with an LDL cholesterol level of ≥100 mg/dL.18)81)
Even if the LDL cholesterol is <100 mg/dL without atherosclerotic cerebrovascular diseases, statin therapy is strongly recommended to improve dyslipidemia in patients with atherosclerotic cerebral infarction or TIA.
There are no sufficient data on the effects of other lipid-lowering agents on the secondary prevention of stroke.
2. Chronic kidney diseases
1) Approach to dyslipidemia in patients with chronic kidney disease
It is evident that the CVD risk is increased in all patients with chronic kidney disease (CKD) regardless of the severity of renal dysfunction.82) However, there are insufficient studies on the usefulness of measuring lipid concentration, how to select the patients for treatment, and its effects.
It is less useful to measure the lipid concentration in evaluating the cardiovascular risk in patients with CKD. In general, higher LDL cholesterol is associated with a higher risk for CVD even in patients with CKD; however, in patients with advanced CKD, who are at a very high risk for CVD, the LDL cholesterol level could be rather low owing to coexisting inflammation or malnutrition. Therefore, there are limitations in determining whether to start treatment on the basis of the LDL cholesterol level.
For an adult with a newly diagnosed CKD (including those with dialysis and transplantation), lipid profiling should be conducted, including total cholesterol, HDL cholesterol, triglycerides, and LDL cholesterol, whereas the follow-up test timing, interval, and method should be determined according to the patient's status.
2) Cholesterol-lowering medication in patients with chronic kidney disease
CKD is considered to have an equivalent risk to CAD, and LDL reduction is the primary target of therapy.3)82)
As subgroup analyses of large clinical studies reported a preventive effect,83)84)85) statin monotherapy or statin/ezetimibe combination therapy is recommended in patients with CKD who are not currently subject to chronic dialysis therapy or those without renal transplantation.
As there was no preventive effect reported in patients with CKD requiring chronic dialysis therapy,85)86)87) statin or statin/ezetimibe combination therapy should not be newly started in those patients.
If patients with CKD requiring chronic dialysis therapy already have received statin or statin/ezetimibe combination therapy at the time of starting dialysis, such treatment can be maintained because a significant beneficial effect was observed in study subjects who did not receive dialysis therapy at the time of research enrollment but started dialysis during the research period, from a subgroup analysis of a large-scale study.85)
There is insufficient data about the safety of high-dose statin therapy in patients with CKD and a glomerular filtration rate of <60 mL/min/1.73 m2. It is recommended to treat with the same dosage as that used in clinical studies, as these patients are at a high risk for potential adverse effects. As decrease in LDL cholesterol and better clinical outcomes were observed in some Asian studies even with relatively lower dosage, lower-dose treatment should be considered.
3) Triglyceride-lowering medication in patients with chronic kidney disease
To improve hypertriglyceridemia in adults with CKD, including patients requiring chronic dialysis therapy and those who had undergone renal transplantation, therapeutic lifestyle modification is recommended. It was reported that fibric acid treatment is associated with an increase in serum creatinine level, related hospitalizations, and nephrologist consultations.88) On the basis of those evidences, it is not currently recommended to use fibric acid in patients with CKD for the purpose of lowering cardiovascular risks.
4) Summary
In reality, there is no consistent answer yet with respect to the effects of statin in patients with CKD. Such controversy is directly due to the shortage of high-quality large-scale studies in patients with CKD. Since the mid-2000s, several large-scale research results have been announced, based on which the guidelines on dyslipidemia in patients with CKD were published in 2013 by the Kidney Disease: Improving Global Outcomes.89)
3. Diabetes
Patients with type 2 diabetes have a 2–3-fold increased risk for cardiovascular mortality than those without diabetes. Therefore, dyslipidemia should be aggressively treated in patients with type 2 diabetes.90)91) The typical pattern of diabetic dyslipidemia is hypertriglyceridemia and reduced HDL cholesterol levels. In addition, even though LDL cholesterol level is not elevated, it is more susceptible to atherosclerosis with more small dense LDL particles. Therefore, it is recommended to measure the blood lipid profile in patients with diabetes at the time of the first diagnosis and annually thereafter. Besides lipid profile (total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides), it is helpful to evaluate diabetic dyslipidemia by measuring the non-HDL cholesterol or apo B level.
The representative study on whether to use statins for primary prevention in patients with type 2 diabetes is Collaborative Atorvastatin Diabetes Study.92) As a result of administering 10 mg atorvastatin to patients with type 2 diabetes aged 40–75 years and with one or more cardiovascular risk factors, the average LDL cholesterol was 72 mg/dL, which was reduced by 39% compared with the baseline, whereas the risk of CVD was reduced by 37%. The meta-analysis also reported that statins decreased CVD by up to 20% in patients with type 2 diabetes when LDL cholesterol was reduced by 1 mmol/L (38 mg/dL), regardless of the baseline LDL cholesterol level.30)
In patients with type 2 diabetes, the first priority of dyslipidemia treatment is to lower LDL cholesterol to <100 mg/dL. In addition, it is recommended to maintain HDL cholesterol at ≥40 mg/dL in men and at ≥50 mg/dL in women, and triglycerides at <150 mg/dL.
This guideline for the management of dyslipidemia classifies patients with CVD as very high-risk patients regardless of diabetes, and recommends more aggressive treatments to control LDL cholesterol. For patients with diabetes without CVD, it is recommended to lower LDL cholesterol to <100 mg/dL.
Patients with diabetes and dyslipidemia should be educated about intensive lifestyle modification.
Statins are recommended first, not only for secondary prevention but also for the primary prevention of CVD in patients with type 2 diabetes.
There is a lack of evidence on the effect of dyslipidemia medications other than statins (omega-3 fatty acids and niacin), owing to insufficient data, especially in domestic studies.
4. The elderly
The prevalence and mortality of CVD are expected to continuously increase because of the increase in the population of elderly persons, especially the very elderly. In particular, the prevalence of dyslipidemia increases in the elderly, who are a high-risk group for CAD, and for whom lipid-lowering therapy will provide many benefits.
The 2013 ACC/AHA guidelines recommend using statins continuously if a person >75 years old has already used it without adverse effects. Use of moderate-intensity statin is recommended, but for secondary prevention. High-intensity statin therapy might not be applicable to the elderly, owing to limited data.4) Statin therapy for primary prevention among the elderly should be determined after considering the comorbidities, safety issues, and priorities of care.
Meanwhile, the ESC/EAS guidelines recommended using statins for the young and the elderly because there was no difference in risk reduction both for primary and secondary prevention. It also recommended to exercise care concerning drug interactions and the adverse effects of statins, because many patients have concomitant diseases or take multiple other drugs.3)
1) Primary prevention
Statins can be beneficial for primary prevention in the elderly people because it was reported to significantly reduce the incidence of CVD and the cardiovascular mortality.66)
2) Secondary prevention
Statin therapy is known to be useful in elderly patients with CVD, with fewer adverse effects than those in young adults.93) The use of statins in elderly patients is considered to be cost-effective.
3) Safety and drug interaction
For elderly patients, the risk of adverse drug reactions caused by statin should be considered. No significant increase in adverse drug reactions has been reported in elderly patients, including rhabdomyolysis and elevated hepatic enzymes; thus, statin can be used safely also in elderly patients.
Statin tends to be less used in elderly patients who require statin therapy owing to concerns about safety and efficacy issues. There are many studies supporting the effect of statins on the primary and second prevention of CVD in the elderly. In particular, the cost-effectiveness of statin therapy is more prominent in elderly patients as they have a higher risk of CVD than young adults.
There are insufficient data on the usefulness and safety issues in the very elderly (≥80 years old), and on whether aggressive lipid-lowering therapy with high-dose statins is helpful in the elderly.
5. Children and adolescents
2) Blood lipid screening test
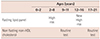
If a blood lipid screening test is conducted in children who have a history of premature CAD or dyslipidemia, it will lead to missing 30–60% of children with dyslipidemia. Therefore, the blood lipid profile should be routinely screened even when there is no clinical or family history.
As total cholesterol and LDL cholesterol decrease by 10–20% during adolescence, the blood lipid profile should be screened routinely in children aged 9–11 years. Non-HDL cholesterol is used for screening the blood lipid profile in children and adolescents.
If children or adolescents have a family history of premature CAD or cardiovascular risk factors, they are considered to have a high risk of developing dyslipidemia, and their blood lipid profile should be screened, as shown in Table 5-2.
3) Treatment of dyslipidemia
Dyslipidemia treatments consist of nonpharmacological and pharmacological therapy, with the priority placed on aggressive nonpharmacological therapy and lifestyle modification. Lifestyle modifications include diet therapy, smoking cessation, and exercise; moreover, education should be aggressively provided to children and their family.
(1) Diet95)
For step 1 (diet therapy), fat should be maintained at about 30% of the total calorie for normal growth and development, whereas the saturated fat intake should be limited to <10% and the total cholesterol intake should be limited to <300 mg (CHILD1 diet).
If the goal is not reached, step 2 diet therapy (saturated fat intake <7%, total cholesterol intake <200 mg daily, trans fat intake <1%, unsaturated fat intake of about 10%) should be conducted (CHILD2-LDL diet).
If the triglycerides increase, monosaccharide intake should be reduced and weight should be reduced. CHILD2-TG diet therapy should be conducted.
(2) Lifestyle modifications
It is recommended to perform exercises with an appropriate intensity on a regular basis, to maintain the proper BMI, as well as to quit smoking with the establishment of an environment for smoking prevention.
(3) Pharmacological therapy96)
If lifestyle modification has been tried for at least 6 months but failed in children and adolescents with dyslipidemia, it is possible to consider medication after evaluating the LDL cholesterol level and the cardiovascular risk level. The fasting blood lipid profile is tested at least twice or at 2 weeks to 3 months interval, to evaluate the need for medication. Medication can be started in children aged 10 years or older in general, except for special cases. The LDL cholesterol goal is at least ≤130 mg/dL in children and adolescents.
Medication should be started under the following conditions:
①If LDL cholesterol is ≥190 mg/dL in children aged 10 years or older who conducted lifestyle modification for >6 months;
②If LDL cholesterol is 160-189 mg/dL in children aged 10 years or older who conducted lifestyle modification for >6 months and have a risk for CVD (if there is a family history of premature CAD, or at least two or more risk factors of CVD).
If the LDL cholesterol is 130-190 mg/dL in children ≥10 years old and not at a risk for CVD, lifestyle modification and controlling BMI under the 85th percentile are recommended.
For medication, adverse effects should be evaluated on a regular basis. The safety issue about long-term statin therapy in children and adolescents has not been well established yet.
Medication may be considered according to the level of LDL cholesterol, presence of CVD risk factors or family history of premature CAD. Medication may be started with statins or fibrate in patients with the TG level >500mg/dL (Fig. 5-1).
6. Familial hypercholesterolemia
The incidence of heterozygous familial hypercholesterolemia (FH) is reported to be 1 per 500 people in Western studies. The most common cause is a mutation of LDL receptor genes, rarely caused by apo B or PCSK9 gene mutation. The LDL cholesterol level is about 200–400 mg/dL in adulthood, whereas the triglyceride level is usually normal, or elevated in some cases. If not treated, half of the male patients and 15% of the female patients might die at the age of about 60 years; however, there is no difference in life expectancy with early treatment.3)97)
1) Diagnosis
FH should be suspected in a patient with a family history of premature CAD in <50 year-old males or in f<60 year-old female or those with a history of FH. Secondary causes of hypercholesterolemia should be ruled out. For the diagnosis, the clinical criteria or DNA analysis is used, and the clinical criteria for diagnosis include the Simon Broome criteria (Table 5-3),98) Dutch criteria,99) and MED/PED criteria.100) It might be identified even in patients without clinical signs such as tendon xanthoma. If a patient has been found to have heterozygous FH, cascade family screening is recommended.
2) Treatment
General considerations: Heterozygous FH management includes the lifestyle modifications, lipid-lowering medication, and tests for atherosclerotic disease. Diet therapy and avoidance of smoking are important lifestyle modifications. Aggressive medication therapy is needed but should be administered with caution in women with a childbearing potential. To decide medication, combined drugs, comorbidities, and adverse effects should be considered, and patients and their family members should be informed of the fact that medication must be continued lifelong. High-dose statin is recommended first, and then ezetimibe can be used in combination or alone when LDL cholesterol level fails to reach the target level
with statin alone or when adverse effects occur.
Target goal of treatment: The goal of LDL cholesterol is same as that in patients with a high risk for CVD. However, a maximal reduction of LDL cholesterol that can be achieved without adverse effects should be the target because it is usually difficult to lower the level to <70 mg/dL in FH, even with the maximum dosage of medication. It is reasonable to lower the LDL cholesterol by ≥50% from the baseline.3)4)
7. Pregnancy
1) Lipid metabolism during pregnancy
(1) Changes in lipid metabolism during pregnancy
Lipids in plasma during pregnancy decrease at the first stage, and then begin to increase after 8 weeks of pregnancy. In the first and second trimesters, fat accumulates owing to increased appetite and lipogenesis; however, fat accumulation decreases during the third trimester owing to the increase in lipolysis and decrease in lipoprotein lipase activity.101)
In the later period of pregnancy, insulin resistance increases lipolysis, glyconeogenesis, and ketogenesis in the fasting state in pregnant women. Insulin increases the activity of lipoprotein lipase in adipose tissue and reduces the activity of hormone-sensitive lipase, which is a lipolytic enzyme. In addition, insulin inhibits hepatic gluconeogenesis and ketogenesis. Peripheral insulin resistance develops in women with gestational diabetes and plays a role in increasing blood nonessential fatty acids and ketone body concentration.102)
(2) Hyperlipidemia during pregnancy
In the later period of pregnancy, triglycerides, phospholipids, and cholesterol increase. In particular, the increase of triglycerides is most prominent. Whereas HDL cholesterol increases in the 12th week of pregnancy due to the increase of estrogen, the total cholesterol and LDL cholesterol increase in the second and third trimesters. Triglycerides increase in VLDL. During pregnancy, hepatic lipase decreases the size of triglyceride-rich LDL cholesterol and increases its density. Such changes damage endothelial cells and cause atheroma formation.
2) Treatment of dyslipidemia during pregnancy
(1) Lifestyle modifications
Physical activity is effective in preventing gestational diabetes and gestational hypertension. The average triglyceride level, of any kind, is lower in women who are physically active. For diet therapy, it is difficult to make a clear conclusion yet, and additional studies are required.
(2) Omega-3 fatty acid
Omega-3 fatty acids belong to the elements of diet, and they are not considered to increase the adverse effects during pregnancy. There are insufficient data to recommend omega-3 fatty acid supplements instead of fish intake to normal pregnant women. However, supplementation of docosahexaenoic acid is recommended in pregnant women who do not usually eat fish at all.
(3) Statins
Statins are contraindicated during pregnancy. Statins are not thought to increase fetal anomalies during pregnancy. Statin therapy is not recommended during pregnancy because there is no evidence that dyslipidemia treatment is beneficial to pregnant women or that cholesterol is required for the growth of embryo during pregnancy. A woman who is planning pregnancy or is already pregnant, should stop statins, if she is taking statins.












 XML Download
XML Download