

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
It is well-known that many hypertensive patients need combination therapy for proper blood pressure (BP) control. Combining two complementary antihypertensive agents has benefits in terms of better response rate and fewer adverse effects.1) When monotherapy is inadequate for BP control, the next step is either to increase the monotherapy dose or to add another antihypertensive agent, usually of a different mechanism; the decision is usually an empirical one made by the physician. A number of studies have been conducted to evaluate the effectiveness of combination therapy of a calcium channel blocker and an angiotensin receptor blocker versus monotherapy of either of 2 drugs when current monotherapy failed to control BP adequately. However, the majority of these studies compared monotherapy and combination therapy that used the same drug dose2)3)4)5)6) or had only a single arm.7)8) Other studies compared valsartan 160 mg with an amlodipine/valsartan combination of either 5/160 or 10/160 mg,9) or they compared monotherapy with combination in various dosages as an initial treatment in stage 2 hypertension.10) Meta-analysis showed that combination therapy in general had much greater BP-lowering efficacy than did doubling the monotherapy dose.11)
A recent study12) compared the outcomes of a doubled-dose angiotensin receptor blocker (olmesartan) with the combination of an angiotensin receptor blocker and a calcium channel blocker. The combination therapy group had significantly but moderately lower systolic blood pressure (SBP; approximately 3 mmHg) in this study, with reduced risk of cardiovascular events only in the subgroup that had preexisting cardiovascular diseases.
This study (COmbination therapy vs. MOnotherapy in DOubled-dose in hypertensive patients with inadequate REsponse to monotherapy, COMMODORE) was designed to answer the commonly encountered, specific clinical question of whether the combination of a calcium channel blocker and an angiotensin receptor blocker (amldopine/valsartan 5/160 mg) is superior to monotherapy with a doubled dose of a calcium channel blocker (amlodipine 10 mg) when the initial conventional dose of the calcium channel blocker (amlodipine 5 mg) has been inadequate in BP control. Because there was a study that showed that amlodipine 5 mg and valsartan 160 mg showed comparable BP reduction,13) this comparison seems to be reasonable.
Subjects and Methods
Study design
This study was conducted as a multicenter, open-label, randomized controlled trial. For the randomization, the following criteria had to be fulfilled: 1) men and women aged 20-80 had to have been diagnosed as having hypertension, 2) they had to have been on monotherapy of amlodipine 5 mg for at least 4 weeks, and 3) their BP had to be inadequately controlled as evaluated by 24-hour ambulatory blood pressure criteria: day-time average SBP≥135 mmHg or diastolic blood pressure DBP≥85 mmHg (SBP≥125 mmHg or DBP≥75 mmHg in patients with diabetes mellitus). Initial screening for enrollment was conducted with both drug-naïve hypertensive patients and patients who were on antihypertensive monotherapy but with inadequately controlled BP (SBP>140 mmHg or DBP>90 mmHg, with diabetes mellitus (DM) SBP>130 mmHg or DBP>80 mmHg). Those who had been already on amlodipine 5 mg monotherapy for more than 4 weeks underwent 24-hour ambulatory BP monitoring, and those who had not been treated by amlodipine were prescribed a 4-week runin treatment of amlodipine 5 mg daily, and 24-hour ambulatory BP was monitored after the run-in treatment period. Eligibility was assessed according to the 24-hour ambulatory BP results. Amlodipine was confined to amlodipine besylate (Norvasc®; Pfizer Inc., New York, NY, USA), and Caduet® (Pfizer Inc., New York, NY, USA) containing amlodipine 5 mg was also acceptable. In the latter case, after the randomization, atorvastatin was prescribed separately, and the dose was maintained during the study period.
The exclusion criteria were as follows:
Severe hypertension (baseline clinic SBP>180 mmHg or DBP>110 mmHg)
Suspicion of secondary hypertension or any severe target organ damage that necessitated urgent BP control
Patients who were "apparently" uncontrolled because of the white coat effect but were actually well-controlled (clinic BP>140/90 mmHg but average home BP or daytime ambulatory BP<135/85 mmHg)
Past history of adverse events on either a calcium channel blocker or an angiotensin receptor blocker
Significant renal insufficiency (serum creatinine>1.5 times upper normal limit) or hepatic insufficiency (aspartate transaminase/alanine transaminase>3 times upper normal limit)
Pregnancy/lactation or planning for pregnancy
Failure to consent
The following medications were prohibited during the whole study period: 1) any antihypertensive agents except for the study drugs and 2) vasodilators that could affect blood pressure, including nitrates. Medications for glucose control and lipid lowering were allowed, but the regimen and dose had to be the same throughout the study period.
Study procedures
The study scheme is shown in Fig. 1. At the initial visit, BP was measured manually as follows: BP was measured in a quiet room with a mercury sphygmomanometer, preferably by the same research nurse throughout the study. Measurements were obtained after the patient had rested in a sitting position for at least 5 minutes, 3 times with the arm resting on the desktop, at 1-minute intervals. When the SBP discrepancy between the first and last measurements exceeded 20 mmHg, an additional measurement was taken, and the first reading was discarded. The average of the three measurements was used. Measurements from both arms were obtained, and when the SBP differences between arms were greater than 10 mmHg, the arm with the higher SBP was used for additional measurements; otherwise, the nondominant arm was used. Clinic BP at the randomization visit was designated as the baseline clinic BP while patients were on daily amlodipine 5 mg.
Reevaluation before randomization was done by 24-hour ambulatory blood pressure monitoring (ABPM) during the last week of the 4-week period of amlodipine monotherapy. ABPM criteria for inadequate control were -5 mmHg of clinic BP criteria, i.e., day-time average SBP≥135 mmHg or DBP≥85 mmHg (SBP≥125 mmHg or DBP≥75 mmHg in patients with DM).
If a patient fulfilled the criteria, randomization to either amlodipine (Norvasc®; Pfizer Inc., New York, NY, USA), 10 mg (group A) or fixed-dose combination of amlodipine 5 mg+valsartan 160 mg (Exforge®; Norvatis Pharmaceutical Co., East Honover, NJ, USA) (group AV) was done using a predefined randomization table for each center. Follow-up visits were made at 4 and 8 weeks. The visit at 4 weeks was to evaluate any condition for stopping the study, such as intolerable side effects, at the researcher's discretion.
Twenty-four hour ABPM was measured during the 8th week after randomization. Monitoring and analysis of the results were performed using each hospital's equipment. Daytime and nighttime settings were: 7:00-22:00 and 22:00-7:00. The minimal frequency of measurements was 30-minute intervals during daytime and 60-minute intervals at night, but a protocol with more frequent measurements, e.g., 15 minutes during daytime and 30 minutes at night was allowed at the researcher's if the patients could tolerate it. Patients were instructed to complete an activity log during the monitoring and to stop all motions during BP measurements. Adequate BP control was defined as daytime average SBP<135 mmHg and DBP<85 mmHg (SBP<125 mmHg and DBP<75 mmHg in patients with diabetes mellitus).
Statistical analysis
The initially planned sample size was 259 for each group with assumed BP reduction for group A and AV being 8.0 and 6.3 mmHg, respectively, and standard deviation 7 mmHg, with alpha error=0.05 and beta error=0.20, non-inferiority margin=5.0.14)15) However, based on the interim analysis results, early termination was selected. Analysis was conducted on an intention-to-treat basis.
The continuous variables were described as mean±standard deviation or median (25-75 percentile) if a variable was not normally distributed. The means were compared between the 2 groups using Student's t-test or Wilcoxon's rank sum test for variables that were not normally distributed. All comparisons were performed with 2-tailed tests. In t-tests with unequal variances between the groups, Satterthwaite degrees of freedom were used. Associations between categorical variables, e.g., comparisons of adverse effects between groups, were tested with the c2 test. p-value below 0.05 was considered statistically significant. Stata/MP 12.1 for Windows (32-bit) (College Station, TX, USA) was used for the statistical analysis.
Results
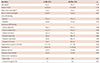
From September 2009 to November 2011, 230 men and women were enrolled in the study from the 10 training hospitals in the Republic of Korea. Nine failed the screening, leaving 221 to be randomized, and 190 completed the 8-week follow-up. Table 1 shows general characteristics of the study subjects. There was no significant difference between groups A and AV. Prevalences of comorbidities such as dyslipidemia, diabetes, coronary artery disease were similar. Baseline clinic and ambulatory BPs did not differ between groups.
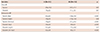
There was significant BP reduction at 8 weeks after randomization in both groups. Both systolic and diastolic sitting blood pressure at the clinic decreased significantly more in the AV group than in the A group. The ambulatory systolic and diastolic BP decreases were significantly greater in the AV group in the daytime and 24-hour average BP decreases were also significantly greater, except for nighttime BP, which showed marginal statistical significance. The difference between the two groups was approximately 5/4 mmHg (Fig. 2 and Table 2). BP control was higher in the AV group than in the A group (30.9 % vs. 14.4 %, p<0.01), when adequate BP control was defined as daytime mean SBP<135 mmHg and DBP<85 mmHg. Based on 24-hour mean BP, the control rate was also higher in the AV group (A group vs. AV group 7.2 vs. 24.5%, p<0.001) using the criteria of adequate control defined as 24-hour mean SBP<130 and DBP<80 mmHg.
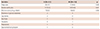
Drop-outs and adverse effects were not significantly different between the two groups (Table 3). Adverse events that were considered to be related to the medication were 6.3 and 4.5% in the A and AV groups, respectively, and common symptoms included dizziness and leg edema. Serious adverse events occurred in 3 subjects but they were not directly related to the clinical trial.
Discussion
We conducted a multi-center, open-labeled randomized controlled trial to investigate whether combination amlodipine/valsartan 5/160 mg was better than amlodipine 10 mg when amlodipine 5 mg had been inadequate in BP control, with blood pressure outcome evaluated by 24-hour ambulatory BP monitoring. The results showed the clear superiority of the combination amlodipine/valsartan 5/160 mg over the doubled dose (10 mg) of amlodipine monotherapy, as shown by the significant difference in reduction of 24-hour, daytime and nighttime mean ambulatory BP values.
Both amlodipine and amlodipine/valsartan combination are commonly used antihypertensive drugs, and the latter are frequently used as a single-pill combination. A number of studies have compared the two agents. However, they did not answer the specific clinical question of whether to double the dose or to add a second agent in case of monotherapy failure. Many studies compared combination therapy with monotherapy continued on the same dose. For example, Ke et al.3) compared amlodipine 5 mg vs. amlodipine/valsartan 5/80 mg in patients whose BP control was inadequate with amlodipine 5 mg, and Schunkert et al.4) compared amlodipine 10 mg vs. amlodipine/valsartan 10/160 mg. Some studies compared valsartan 160 mg with amlodipine/valsartan 5/160 and/or 10/160 mg.6)9) Other studies had only a single arm.7)8) There was one study with a similar design that showed the superiority of combination therapy,16) but it used mean sitting BP as an outcome. None of the related studies utilized 24-hour ambulatory BP monitoring, and our data show the better efficacy throughout 24 hours including nighttime.
In our data, combination treatment showed ambulatory systolic BP≈5 mmHg lower than that from high-dose monotherapy, which was a slightly larger difference compared with the result of a similar study that compared the difference of ≈3 mmHg between olmesartan 40 mg and amlodipine or azelnidipine/olmesartan 20 mg combination. This study reported outcome improvement in combination treatment in the subgroup with preexisting cardiovascular diseases, although the overall analysis showed no significant differences.
Some studies have shown the benefits of combining calcium channel blockers and angiotensin receptor blockers or angiotensin-converting enzyme inhibitors with amelioration of vasodilatory side effects of the former by the latter.14)17) However, drug-related adverse effects were not significantly different between the two groups in this study; it is likely that our study was underpowered for detecting differences in adverse effects. Although drug-specific side effects tended to be common in the high-dose amlodipine group, such as leg edema, hot flashes, and palpitation, which are typical vasodilatory side effects of calcium channel blockers, the drug-related adverse effects in the amlodipine/valsartan combination group were mainly dizziness, which likely reflected greater BP reduction.
There is a possibility that concomitant medications, such as statins, can influence BP control. However, as shown in Table 1, the proportion of statin usage was not different between the two groups.
One drawback of this work is that comparing amlodipine 10 mg with amlodipine/valsartan 160 mg may be "unfair," and there is an argument to be made that amlodipine/varsaltan 5/80 mg is a more appropriate counterpart. Unfortunately, we had no choice in this issue because the amlodipine/valsartan 5/80 mg combination pill was not available in the majority of the participating institutions at the time of the initial planning of the study.
There are a number of other limitations. The equipment for ambulatory BP monitoring and analysis was not uniform but instead varied by participating institution, and information collected on comorbidity was not shared. Additionally, many of the enrolled patients had been recently diagnosed with hypertension, and this population may not have represented patients with long-standing hypertension. Some of the routine procedures for randomized controlled trials were not strictly followed, such as wash-out and placebo run-in periods. Medication before the randomization was not identical because both Norvasc® (Pfizer Inc., New York, NY, USA) and Caduet® (Pfizer Inc., New York, NY, USA) were used, although Caduet was used in only two cases.
In conclusion, amlodipine/valsartan 5/160 mg was more efficacious than amlodipine 10 mg in hypertensive patients in whom monotherapy with amlodipine 5 mg had failed, and thus, the combination treatment may be preferred in this clinical setting.


 XML Download
XML Download