

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Primary mitral valve regurgitation (MR) is the second most common type of valvular heart disease.1)2) Severe degenerative MR is associated with increased risk of morbidity and mortality, but prognosis is improved with successfull surgery.3) However, the optimal timing of surgery in patients with severe MR remains controversial.4)5) According to the European and American College of Cardiology/American Heart Association guideline recommendation,1)2) mitral valve repair must be proposed to symptomatic patients and to patients with significant left ventricular (LV) remodeling as a consequence of MR severity. A significant decline in LV function is defined, in these recommendations, echocardiographically as an LV ejection fraction (LVEF)<60% or an LV end-systolic diameter (LVESD)>40 mm. Preoperative LV systolic function and LVESD are important postoperative measures.6) However, it is still difficult to decide when a patient should be referred for surgery.7)8) MR causes low LV afterload and the ejection fraction thus remain normal or supernormal until the disease reaches an advanced stage. Thus, the interpretation of LVEF in the significant MR may be difficult.9) Strain analysis has been used as a quantitative approach to accurately estimate regional myocardial contractility in various diseases. The LV wall is not homogenous and is composed of 3 layers of fibers. LV function is determined by the sum of contraction and relaxation within these 3 layers.10) Two-dimensional multilayer speckle-tracking echocardiography (2D MSTE) can be used for the early detection of LV systolic and diastolic dysfunction in these 3 each layers. 2D MSTE can be used for the early detection of LV systolic and diastolic dysfunction in patients with ischemic or non-ischemic heart disease and normal LVEF.11)
The aim of this study was to evaluate the predictive value of preoperative regional LV contractile function assessment using two-dimensional multilayer speckle tracking echocardiography in patients with chronic severe MR with normal LV systolic function.
Subjects and Methods
Patient selection
Forty-three patients with severe primary MR, LVESD<40 mm, and preserved LVEF>60% scheduled for mitral valve replacement or repair were enrolled between January 2007 and June 2014. The severity of MR was determined by an integrated echocardiographic evaluation using the following measurements: LV dimension, effective regurgitant orifice (ERO), and regurgitant volume (RV). Severe MR was defined as ERO>40 mm or RV>60 mL.1)2) Exclusion criteria included secondary MR due to distortion of the subvalvular apparatus or secondary to LV enlargement and remodeling (idiopathic cardiomyopathy or ischaemic heart disease), other concomitant valvular disease of moderate or severe severity, coronary artery disease defined as >50% narrowing in at least one coronary artery in a previous angiogram, history of myocardial infarction, coronary artery bypass graft, acute coronary syndrome, atrial fibrillation, chronic renal failure, or suboptimal imaging. Medical records were carefully reviewed by a single investigator (Cho EJ) to determine the presence of symptoms and comorbidities. Chronic kidney disease was defined an estimated glomerular filtration rate of less than 60 mL/min/1.73 m2.12) Smokers were defined as patients documented to be current smoker at time of clinical evaluation. The presence of symptoms was defined as the New York Heart Association Functional Classification of more than grade 2. In this study, we defined remodeling after MVR by a decrease of longitudinal global longitudinal strain (GLS) or LVEF that did not decrease LV end-diastolic dimension (LVEDD). The study subjects were then divided into 2 groups: those with a reduction in LVEF or increase of LVEDD at 3 months compared to baseline (remodeling group), and others (non-remodeling group).
The regional ethics committee approved the study. The patients provided informed consent before being enrolled in the study.
Clinical assessment and N-terminal of the prohormone brain natriuretic peptide
Demographic information was collected from standardized questionnaires by the study cardiologist at the time of enrollment. We obtained a baseline medical history, medications, weight, height, pulse, blood pressure, electrocardiography (ECG), and baseline blood measurements.
Blood samples were taken from the antecubital vein into tubes containing lithium heparin and then centrifuged. Serum samples were separated and stored at -70℃ until further analysis. Plasma NT-pro BNP levels were measured using an Elecsys pro BNP reagent kit and an Elecsys 2010 chemistry analyzer (Roche Diagnostics, Indianapolis, IN, USA). Laboratory operators were blinded to patient identity and characteristics.13)14)
Echocardiography
Two-dimensional echocardiography was performed using commercially available equipment (Vivid 9; GE Medical Systems, Milwaukee, Horten, Norway). End diastole was defined as the frame with the largest cavity area immediately before the onset of the QRS and end systole as the frame with the smallest cavity area. LVEDD, LVESD, diastolic interventricular septum thickness, and diastolic LV posterior wall thickness were obtained from the parasternal views according to standard guidelines.15) LV mass (LVM) was calculated from linear dimensions using the American Society of Echocardiography recommended formula. Left atrial (LA) volume was measured at end-systole from the frame just preceding mitral valve opening using the biplane area length method in the apical 4-and 2-chamber views and was indexed to body surface area.15) LV diastolic function was assessed by the early (E wave) and late (A wave) transmitral velocities, corresponding E/A ratio, and E wave deceleration time using pulsed-wave Doppler (Vivid 9; GE Medical Systems, Milwaukee, WI, Horten, Norway). Tissue doppler imaging was used to measure peak early diastolic mitral annular velocity (e') at the septal mitral annulus in apical 4-chamber view. E/e' ratio was calculated to noninvasively estimate LV filling pressure.16) We used the average of three consecutive Doppler signals to perform these measurements.
Quantitative and qualitative measures of MR severity were made according to the American Society of Echocardiography guidelines.17) MR regurgitant volume was calculated using the proximal isovelocity surface area (PISA) method. The ERO was determined by dividing the regurgitant flow rate, calculated as 2 πr2'aliasing velocity, where r is the PISA radius, by peak MR velocity.17) The jet morphology was also classified by the spatial distribution within the LA: eccentric jets were directed toward the lateral or septal LA walls or along the mitral valve leaflets. Central jets originated from the middle of the mitral valve and did not strike atrial walls or mitral valve leaflets.18)
Two-dimensional multilayer speckle-tracking echocardiography
Analysis of the parasternal short-axis and apical 2D MSTE images was performed offline on a personal computer with the aid of a software package (EchoPAC, GE Ultrasound, Haifa, Israel). Loops of three consecutive cardiac cycles for 2D MSTE images were acquired. Two-dimensional data were analyzed offline using EchoPAC version 113.0.4 (GE Vingmed Ultrasound AS, Horten, Norway) by an experienced investigator blinded to the clinical information in severe MR patients. Speckle-tracking analysis was performed using dedicated wall motion tracking software: Automated Function Imaging for 2D imaging (from GE Vingmed Ultrasound AS, Horten, Norway). Briefly, automatic endocardial delineation was obtained after manual positioning of the end-systolic endocardial border mitral plane and left ventricular apex. The position and size of the region of interest were adjusted manually to provide optimal frame-by-frame wall tracking throughout the cardiac cycle. For strain processing, the peak of the R wave on the electrocardiogram was used as the reference time point for end-diastole. Segments with poor-quality tracking or that provided aberrant curves despite manual adjustment were discarded from analysis. Longitudinal strain (LS) and circumferential strain (CS) were computed from the 2D data set. GLS and CS were obtained by averaging regional strain curves (16-segment model for 2D MSTE ). For all strain components, peak systolic and time to peak strain were defined using regional strain curves.
In addition by 2D MSTE , all three acquired parasternal short-axis and apical views were analyzed using the system to obtain quantitative function parameters for each segment in an 18 segment LV model (six segments at each LV level).19)
Follow –up
Data were obtained until June 2014 (mean follow-up duration: 23.3 months) from regular visits to the outpatient clinic or by telephone interviews. Particular care was taken to obtain information regarding development of symptoms, eventual MV repair or replacement, and deterioration in LV function.
Statistical analyses
Continuous variables are listed as their mean values. Categorical variables are presented as frequencies and group percentages. Continuous variables were compared using the student t-test. The Chi-square or Fisher's exact test was used for comparison of categorical variables. A 2-tailed p<0.05 was considered statistically significant. Pearson's correlation coefficient (r) and intra-class correlation coefficient (ICC) were calculated to express agreement between the strains defined using 2D MSTE. The receiver-operating characteristic (ROC) curve of global, longitudinal area strain by 2D MSTE was calculated for the distinction between two groups. The inter-observer agreement was demonstrated by calculating the coefficient of variation of repeated measurements and ICC. p<0.05 was considered significant. Data analysis was performed utilizing SPSS version 18.0 (SPSS, Chicago, IL, USA).
Observer agreement
The ICC was used to determine the intra and inter-rater reliability, with its respective 95% confidence interval. The ICC showed excellent intra and inter-rater values for measurement of 2D MSTE (intra-rater, ICC 0.942, 95% ICC ranged from 0.879 to 0.973, inter-rater, ICC 0.927, 95% ICC ranged from 0.846 to 0.965).
Results
Analysis of baseline characteristics and echocardiography
The patients' mean age was 51.7±14.3 years and 25 (58.1%) were male. The study subjects were divided into 2 groups: those with a reduction in LVEF or increase of LVEDD at 3 months compared to baseline (remodeling group), and others (non-remodeling group). Baseline characteristics and echocardiographic parameters of the patients with severe MR group are shown in Table 1 and 2. Patients with LV remodeling group had higher creatinine levels than did patients within LV non-remodeling group (p=0.002). When comparing the two groups, the level of NT-pro BNP did not appear to differ. Baseline and post-operative medications were not different between the two groups. Patients with LV remodeling group were more often treated with diuretics.
In examining the echocardiographic parameters between the two groups, the interventricular septal wall thickness, LV posterior wall thickness, left ventricular mass index, left atrial volume index, relative wall thickness (RWT) and E/e' ratio were not significantly different (Table 2).
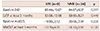
The fraction of individuals who received mitral valve repair or mitral valve replacement did not differ between the two groups (Table 1). Moreover, we analyzed baseline LVEF, midGLS, at least 3 months follow-up LVEF, and at least 3 months follow-up midGLS in two groups; the MV repair group and MVR group. There was no difference between the MV repair and MVR groups on these variables. (Table 3)
Analysis of postoperative echocardiography at 7 days and 3 months follow-up
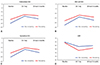
In the postoperative echocardiography at 7 days follow-up, patients with LV remodeling group had larger LVEDD, LVESD, and dimension of LA than did patients with non-remodeling group (p=0.017, p=0.023, p=0.003). Postoperative LVEF was decreased compared to baseline LVEF. However, LVEF was not different between the two groups (p=0.060) (Table 2 and Fig. 1).
At 3 months follow-up, patients within the LV remodeling group had larger LVEDD than did patients with no-remodeling (p=0.047) (Table 2 and Fig. 1). In addition, patients in the LV remodeling group had a higher E/e' ratio than did patients within the non-remodeling group (p=0.019). Postoperative LVEF than baseline LVEF was decreased. However, LVEF was not different between the two groups (p=0.249) (Table 2).
Strain analysis between non-remodeling and remodeling group
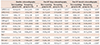
By the 2D MSTE, patients within the LV remodeling group had lower epicardial layer GLS, midlayer GLS, and endocardial layer GLS than did patients within the non-remodeling group (p<0.001, p<0.001, p<0.001). 2D GLS values decreased from the endocardial layer toward the epicardial layer in both two groups (Table 2 and Fig. 2). Postoperative GLS at 7 days follow-up was decreased compared to baseline GLS. Patients within the LV remodeling group had a lower epicardial layer GLS, mid-layer GLS and endocardial layer GLS than patients with non-remodeling group (p=0.001, p=0.021, p=0.016), which was similar to the baseline results (Table 2 and Fig. 2). Postoperative GLS at 3 months follow-up was higher than postoperative GLS at 7 days follow-up. Three-layer's GLS were also decreased in patients within the LV remodeling group than patients within the non-remodeling group (Table 2 and Fig. 2). Postoperative LVEDD and postoperative LVEF were correlated with baseline mid-layer GLS (Fig. 3).
Independent predictors of postoperative left ventricular remodeling in patients with severe mitral valve regurgitation
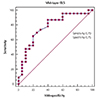
In the present study, study subjects were divided into 2 groups: those with a reduction in LVEF or increase of LVEDD at 3 months compared to baseline (remodeling group), and others (non-remodeling group). ROC curve analysis revealed that the most useful cutoff value for discriminating between patients with LV remodeling and patients with LV non-remodeling in severe MR with normal LV systolic function was -20.5% of 2D mid-layer GLS (sensitivity 0.70, specificity 0.75). (Fig. 4) In addition, as assessed using a ROC analysis, the GLS by 2D MSTE to detect early LV remodeling was a predictive power in patients with severe MR. In multivariable analysis, the baseline mid-layer GLS (95% confidence interval, 1.259-4.729; p=0.008) was independently associated with postoperative LV remodeling or LV dysfunction (Table 4).
Discussion
The main finding of our study in patients with degenerative severe MR and preserved LV systolic function, was that, (1) in the postoperative echocardiography at 7 days follow-up, patients with LV remodeling had larger LVEDD, LVESD, and left atrial dimensions than patients within the non-remodeling group. (2) In the postoperative echocardiography at 3 months follow-up, patients within the LV remodeling group had larger LVEDD than patients within the non-remodeling group (p=0.047). E/e' ratio was higher in patients with LV remodeling group compared to the non-remodeling group. Postoperative LVEF was decreased compared to baseline LVEF. However, LVEF was not different between the two groups. (3) By the 2D MSTE, patients with LV remodeling had lower epicardial layer GLS, mid-layer GLS, and endocardial layer GLS than patients within the non-remodeling group. (4) The baseline mid-layer GLS was an independent predictor of postoperative LV remodeling or LV dysfunction.
Change in left ventricular size and postoperative left ventricular remodeling or dysfunction in patients with severe degenerative mitral valve regurgitation
In generally, several authors have suggested that preoperative LVEF and LVESD are important predictors of postoperative LVEF. In addition, there is also substantial debate regarding the timing of operation to optimize long-term ejection fraction recovery.20)21) The favorable effect of successful mitral valve corrective surgery on LV performance is mainly manifested by a significant decrease in LV size, immediately after the operation and over time during long-term follow-up.3)21) In the present study, the LVEDD of the remodeling group was larger than in the non-remodeling group in echocardiography at 7 days follow-up after the operation and at least 3 months follow-up after the operation. And the degree of decrease in LVEDD between baseline echocardiography and postoperative follow-up echocardiography was larger than in the non-remodeling group. Thus, the postoperative degree of decrease in LVEDD might be an additive predictive factor for postoperative LV dysfunction or remodeling.
Early detection of postoperative left ventricular remodeling or dysfunction in patients with severe degenerative mitral valve regurgitation
In patients with severe MR, the increase in LV wall stress leads to progressive myocardial damage, which ultimately results in myocardial dysfunction. Moreover, a previous study showed that significant histological alterations of myocardial structure and functions are present in patients with severe MR and LVEF>60%.22) Despite successful surgical procedure and careful adherence to current recommendation, postoperative LV dysfunction and clinically evident heart failure may still occur. Conventional echocardiographic parameters fail to detect potential subclinical myocardial damage due to the low sensitivity and to its volume-dependency.22) Therefore, the attention has shifted towards identifying new parameters that would be able to detect subclinical changes in LV myocardial dysfunction. Recently, LV deformation(strain) parameters as assessed with different imaging techniques have been proposed to predict LV dysfunction after mitral valve surgery.23)24) In a previous study, LV GLS showed a significant reduction in disease progression and LV dilatation, even in the presence of normal LVEF. This suggests a promising role of this parameter for the detection of LV dysfunction at an early stage before major and irreversible damage of the myocardium occurs.25)
The LV wall is not homogenous and is composed of 3 layers of fibers. The LV myocardium consists of circumferential fibers in the mid-wall layer and longitudinal fibers in the endocardial and epicardial layers. Myofiber orientation changes continuously in the form of a right-handed helix in the subendocardium to a left-handed helix in the subepicardium.26)27)28) Therefore, LV strain is not uniform over the left ventricle; it varies through myocardial layers and levels with circular and longitudinal inhomogeneity. Manaka et al.29) demonstrated that myocardial systolic impairment may originate at the endocardial side and extend to the epicardium. Therefore, differentiation of endocardial, mid-wall, and epicardial strain might be a novel method for assessing LV mechanics in cardiovascular disease. 2D MSTE can be used for the early detection of LV systolic and diastolic dysfunction in these 3 each layers. By the MSTE at baseline echocardiography, patients with LV remodeling had lower epicardial layer GLS, mid-layer GLS, and endocardial layer GLS than did patients within the non-remodeling group. And postoperative LVEDD and postoperative LVEF were correlated with preoperative mid-layer GLS. Therefore, baseline mid-layer GLS was a powerful predictor of long-term LV dysfunction after MV reconstruction or replacement, even when adjusted for other well-established prognostic factors. To the best of our knowledge, this was the first study to evaluate the predictive value of postoperative LV dysfunction using 2D MSTE in primary chronic severe MR with preserved LV systolic function. GLS might be provided an important additional tool for the monitoring and management of patients with severe MR.
Limitations
Several potential limitations of our study must be noted. Firstly, this was a single-center study that included a relatively selected population of patients with primary severe MR without concomitant other valve disease. Consequently, the sample size was relatively small. Therefore, large-scale multicenter prospective studies are needed to clarify the additive prognostic implications of 2D MSTE. Secondly, this study was performed using prospective registry data, thus we could not collect or adjust the total duration of medications, which could affect outcomes. In addition, further data on the clinical outcome of such patients should be obtained from complimentary studies with extended follow-up. Finally, we were only able to interrogate the LV dysfunction using 2D ECG and 2D MSTE. Therefore, future studies of the multimodality image study such as cardiac MR are needed to assess the LV dysfunction of these clinical determinants. In addition, future studies comparing the result of multimodality imaging and the result of 2D MSTE are needed to assess the LV dysfunction.
Conclusions
2D MSTE may be used to predict a decrease in LV function following mitral valve replacement or mitral valve repair in patients with chronic primary severe mitral regurgitation with normal LV systolic function. This promising method could be of use in the clinic when trying to decide upon the optimum time to schedule surgery for such patients. Furthermore, the postoperative degree of decrease in LVEDD might be an additive predictive factor for postoperative LV dysfunction or remodeling. When myocardial deformation begins to decrease, surgery should be contemplated even though patients may show little to no symptoms; these methods may help prevent irreversible systolic dysfunction in the long term.



 XML Download
XML Download