

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Current prevention guidelines focus on low-density lipoprotein (LDL) cholesterol lowering as the primary target of therapy, primarily by statins.1) However, many statin-treated individuals continue to experience cardiovascular events.2)3)4)5) Even after low LDL cholesterol levels (70-100 mg/dL) are achieved, residual cardiovascular risk is observed in the randomized clinical trials of high dose statins.2)5) For further reduction of residual cardiovascular risk, physicians should pay attention to modifiable risk factors such as hypertriglyceridemia, non-high-density lipoprotein (HDL) cholesterol, apolipoprotein B, low HDL cholesterol, visceral fat, and insulin resistance. As one of the correctable residual cardiovascular risk factors, hypertriglyceridemia is recently reemerging as one of the reliable therapeutic targets. In Asians, such as Koreans, Chinese, and Japanese, the prevalence of hypertriglyceridemia is greater than hypercholesterolemia within the Korean population,6)7)8) Chinese National Survey,9) and Japanese men (http://www.mhlw.go.jp/bunya/kenkou/eiyou/h25-houkoku.html). In addition, a 2007 Korean National Survey also revealed 33.2% of the general population had hypertriglyceridemia (triglycerides≥150 mg/dL) and 50.2% of them showed low HDL cholesterol levels (men<40 mg/dL, women<50 mg/dL).10) It is important to mention that recent genetic studies and randomized trials demonstrated that low HDL cholesterol might not be a cause of cardiovascular disease and hypertriglyceridemia and remnant cholesterol may be a cause.11) In this review, we reviewed updated evidence of the role of hypertriglyceridemia and triglyceride-rich lipoproteins (TRLs), remnant cholesterol as cardiovascular risk factors and the therapeutic target for reducing residual cardiovascular risk.
Recent Evidence of the Role of Hypertriglyceridemia and Triglyceride-Rich Lipoproteins as Cardiovascular Risk Factors
Experimental evidence
TRLs are too large to enter into the arterial intima and therefore cannot lead to development of atherosclerosis at greatly elevated triglycerides (TG) concentrations (>4450 mg/dL). By contrast, at mild to moderately raised TG concentrations (178-890 mg/dL), TRLs are small enough to enter into the arterial wall and thus have the potential to accumulate and cause atherosclerosis.11)12)13)
TRLs include chylomicrons, very large density lipoprotein (VLDL) and intermediate density lipoprotein (IDL). Their major protein component is apolipoprotein B. In the fasting state, only VLDL and IDL are present in plasma, whereas chylomicrons, VLDL and their remnants circulate under non-fasting conditions. TRLs undergo intravascular hydrolysis by lipoprotein lipase in the muscle, adipose tissue, heart and other tissues, where they provide free fatty acids for energy or storage. Upon lipolysis, chylomicrons and VLDL are depleted of TG and enriched in cholesterol, resulting in the formation of chylomicron remnants and VLDL remnants. In addition, their cholesterol content is further enhanced by the action of cholesterol ester transfer protein (CETP). Since most cells can degrade TG, and there are not any cells that can degrade cholesterol, the cholesterol content of TRLs is more likely to be the cause of atherosclerosis and cardiovascular disease rather than raised TG per se. Indeed, cholesterol, rather than TG accumulates in intimal foam cells and in atherosclerotic plaques, and remnant lipoproteins, much like LDL can enter the arterial intima. In contrast, chylomicrons are too large to enter. Lipoprotein lipase activity at the surface of remnant particles, either at the surface of vascular endothelium or within the intima, leads to liberation of free fatty acids, monoacylglycerols, and other molecules, each of which could cause local injury and inflammation. Although other possible mechanisms have been suggested, perhaps the simplest chain of events is that high triglyceride concentrations are a marker for raised remnants rich in cholesterol, which, upon entrance into the intima, leads to low-grade inflammation, foam cell formation, atherosclerotic plaques, and ultimately cardiovascular disease and increased mortality. (Fig.).11)1213)14)15)
Remnant cholesterol is the cholesterol content of TRLs (chylomicron remnants, VLDL, and IDL) in the fasting or non-fasting states. Because a direct assay that measures all remnants at the same time has not yet been developed, remnant cholesterol can be calculated as non-fasting total cholesterol minus HDL cholesterol minus LDL cholesterol.11) A recent study has shown that remnant cholesterol levels in TRLs are causal in ischemic heart disease independent of reduced HDL cholesterol.16) Because the level of TG is significantly correlated with the amount of remnant cholesterol in TRLs (r=0.96), the amount of TG may represent the level of remnant cholesterol.16) Therefore, the level of TG is a biomarker for circulating TRLs and their metabolic remnants.17)
TRLs drive atherothrombosis via a number of mechanisms. Particle size is a key limiting factor influencing the retention of apolipoprotein B containing lipoproteins. Although large chylomicrons (70 nm diameter) do not penetrate the arterial wall, smaller remnants of chylomicrons and large VLDL, as well as LDL and lipoprotein (a) enter the arterial wall and therefore enhance cholesterol accumulation directly.18) These TRL remnant particles contribute directly to plaque formation and progression.19) In addition, TRLs promote endothelial dysfunction by increasing immune inflammatory responses and destabilize plaque, enhance thrombus formation, promote secretion of tissue factor, fibrinogen, coagulation factors VII, XII, impair fibrinolysis, and increase plasminogen activator inhibitor-1 secretion.19)20)21)22)23)24)
Epidemiologic evidence
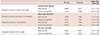
Previous studies have shown that elevated fasting and non-fasting hypertriglyceridemia or very low-density lipoprotein cholesterol were associated with increased risk of coronary heart disease, even after adjustment for HDL cholesterol concentrations.9)25)26) Recent studies demonstrated that raised TG was strongly associated with increasing risks of cardiovascular disease. Raised non-fasting TG was strongly associated with increasing risks of myocardial infarction, ischemic heart disease, ischemic stroke, and all-cause mortality.27)28)29)30) Raised fasting and non-fasting TG were associated with an increased risk of coronary heart disease in an Emerging Risk Factors Collaboration study.31) This association was attenuated after adjustment for HDL cholesterol and non-HDL cholesterol. In multivariate analyses, the relationship between TG and cardiovascular diseases (CVD) is either attenuated or lost, thereby suggesting that the cholesterol content of TRLs or remnant cholesterol is causative for CVD rather than raised TG itself. In addition, data from three major Danish studies provides support for remnant cholesterol in TLRs as a causal factor for CVD by Mendelian randomization study.9)16)30) In these studies, a 39 mg/dL increase in non-fasting remnant cholesterol was associated with a 2.8 fold causal risk for ischemic heart disease which was higher than for observational data alone (hazard ratio 1.4, 95% confidence interval 1.3 to 1.5) and independent of HDL cholesterol concentration.16) These genetic studies reinforce the role of remnant cholesterol in TRLs rather than TG as a cardiovascular risk factor (Table 1). For non-fasting remnant cholesterol alone, for the ratio of non-fasting remnant cholesterol to HDL cholesterol, and for LDL cholesterol alone, causal risk estimates for genetically elevated levels were in the same direction and higher than corresponding risk estimates for corresponding increases in conventional plasma levels of the same lipoproteins; however, this was not the case for HDL cholesterol alone.16) These results demonstrated the important role of non-fasting remnant cholesterol, the ratio of non-fasting remnant cholesterol to HDL cholesterol, LDL cholesterol on the risk of ischemic heart disease than HDL cholesterol in general population.
Remnant cholesterol was causative for ischemic heart disease independent of HDL cholesterol levels (Table 2).32) In these studies, remnant cholesterol was estimated indirectly as total cholesterol minus the cholesterol contents of LDL and HDL. These population based studies clearly demonstrated a role of non-fasting TG and remnant cholesterol levels on the predictions of CVD events in general population. In the statin era, among patients receiving statin therapy after acute coronary syndrome, on-treatment TG≤150 mg/dL was associated with a lower risk of recurrent coronary heart disease events independently of the level of LDL cholesterol.33) Among patients with acute coronary syndrome treated effectively with statins, fasting TG predicts long-term and short-term cardiovascular risk.33) These data support the concept that achieving both low LDL cholesterol and low TRLs may be important therapeutic goals in patients following acute coronary syndrome.
Genetic evidence
The genetic basis of mild to moderate hypertriglyceridemia with or without elevated LDL cholesterol in most individuals is polygenic. Postprandial TG metabolism abnormalities are strongly associated with single nucleotide polymorphisms at common genetic loci. Candidate genes associated with postprandial lipemia include apolipoprotein A1, A4, A5, C3, E, lipoprotein lipase, fatty acid binding protein 2, microsomal transfer protein (MTP), scavenger receptor B1, Angiopoietin-like proteins (ANGPTL)4 and peroxisome proliferator-activated receptor (PPAR) α.32)34)
Recent Mendelian randomization studies with genetic variants reported several candidate genes that affect the concentrations of remnant cholesterol. The relative risks of remnant cholesterol on ischemic heart disease and all-cause mortality according to causal genetic variants compare with corresponding observational results are shown in Table 3.
Lipoprotein lipase (LPL) is the key TG regulating enzyme, which hydrolyzes TG in the circulation and promotes the hepatic uptake of TRLs. A common gain of function LPL variant, S447X, confers an anti-atherogenic lipid profile characterized by low levels of TG and lower incidence of vascular disease or myocardial infarction.35)36) In contrast, several loss of function LPL variants associated with elevated TG levels which have been associated with increased coronary artery disease (CAD) risk.37)38) It was identified as common non-coding variants at the LPL gene locus associated with both TG and CAD risk in the same direction by genome wide association studies.3940)41) Beyond LPL itself, common variants that influence TG levels are significantly associated with CAD risk even after adjusting for their effects on other lipid traits.42) Among the common variants with strong associations with both TG and CAD were those at a gene locus containing the genes apolipoprotein C3 (APOC3) and apolipoprotein A5 (APOA5) which encode apoC-III and apoA-V, respectively, and are found on TRLs and known to be the regulators of LPL activity and TG levels.43)
ApoC-III is a key regulator of fasting and postprandial plasma TG levels and TG homeostasis. It is synthesized principally in the liver and expressed in the liver and intestine and circulates on and exchanges between TRLs and HDL.44)45) ApoC-III inhibits LPL-mediated hydrolysis of TRLs and adversely affects receptor-mediated hepatic uptake of remnants of TRLs.45) At higher concentrations, ApoC-III also inhibits the activity of hepatic lipase, an enzyme that plays an important role in the conversion of VLDL to IDL and LDL, as well as in the remodeling of HDL. Thus, elevated levels of ApoC-III in plasma have been associated with both impaired lipolysis and impaired clearance of TRLs from the circulation, which results in the accumulation of atherogenic VLDL and chylomicron remnants.45) Furthermore, some study suggested that ApoC-III has direct proinflammatory effects at the level of the vessel wall.46)47) Elevated ApoC-III levels are an independent risk factor for cardiovascular disease and genetic variants that result in a loss of function and attenuated levels of ApoC-III in plasma are associated with a reduced risk of coronary heart disease.45)48)
APOA5 is thought to play a crucial role in TG metabolism. APOA5 knockout mice demonstrate profound TG, whereas human APOA5 transgenic mice have significantly lower plasma TG than controls.51) Studies of APOA5 have revealed several coding variants have been implicated in severe hypertriglyceridemia or hyperchylomicronemia and some common coding variants have also been attributed to increased CAD risk.52)53)54) In addition, carriers of rare non-synonymous mutations at APOA5 were at a 2.2 fold increased risk for myocardial infarct when compared with non-carriers.55) Analysis of a specific APOA5 variant (1131T>C) that regulates pathways of TG metabolism showed an association with coronary risk. The increase in risk per allele was also concordant with data from observational studies.56) Taken together, these recent studies have provided powerful evidence that plasma levels of TRLs are causally related to the development of CAD and specifically that apoC-III promotes and APOA5 protects against CAD.43) In addition, these offer strong support to the hypothesis that intervention to lower TRL levels may decrease the risk of CAD.
Taken together, genetic studies strongly support the theory that high concentrations of TRLs or remnant cholesterol are causal risk factors for cardiovascular disease and all-cause mortality, and that low HDL cholesterol might merely be a long-term marker of raised TG and remnant cholesterol.11)
Recent Evidence on Hypertriglyceridemia and Remnant Cholesterol as a Therapeutic Target for Reduction of Residual Cardiovascular Risk
General measure and lifestyle interventions
First, secondary causes of hypertriglyceridemiasuch as nephrotic syndrome, alcohol, or obesity should be ruled out and treated. In addition, intensive lifestyle intervention is the fundamental first step in the management of patients with hypertriglyceridemia or cardiometabolic disease. This includes to smoking cessation, increased physical activity, adoption of a Mediterranean style diet, replacing saturated fats with unsaturated ones, reduction of carbohydrate content in the diet, avoidance of refined sugar and fructose, increased intake of complex carbohydrates with high soluble fiber, weight loss and limited alcohol intake. If TG levels remain elevated, pharmacological approaches including fibrates and omega-3 fatty acids are considered.
Treatment options for hypertriglyceridemia and remnant cholesterol
Fibrates and omega-3 fatty acids
Fibric acid is a synthetic ligand of the nuclear receptor PPAR α that is highly expressed in skeletal muscle and the heart where it promotes β-oxidation of fatty acids to mediate hypolipidemic actions. PPAR α regulates expressions of key proteins involved in atherogenesis, vascular inflammation, plaque stability, and thrombosis.57)58) Thus, PPAR α may exert direct anti-atherogenic actions in the vascular wall. Fibrate, PPAR α agonist, therapy significantly improves the lipoprotein profile and the flow-mediated dilator response to hyperemia, reduces levels of inflammatory markers, increases adiponectin levels, and improves insulin sensitivity.57)58)59)60) The beneficial effects of fibrate on endothelial function, inflammation, and insulin sensitivity are highly relevant to CVD and are likely to simultaneously improve both cardiovascular and metabolic health in patients with hypertriglyceridemia. Fibrate therapy improved clinical outcomes in primary and secondary prevention trials especially in patients with low HDL cholesterol and high triglycerides, despite the use of established therapy.61)62)Although the combination of statins and gemfibrozil is more likely to be accompanied by myopathy due to significant pharmacokinetic interactions with statins,63) fenofibrate showed no significant side effects with combination treatment with statins.64)65) Fenofibrate did not reduce events overall in the trials, except in patients with high triglycerides and low HDL cholesterol subgroups. However, the failure of fenofibrate in other patients has been blamed due to several issues such as pretty low triglycerides levels.11) On the other hand, we discussed off-target effects of fibrates such as anti-inflammatory effect.5758)59)60) Indeed, while fibrates appear to work, their benefit does not associate with TG lowering. In other words, a high TG patient may be more likely to benefit, but not necessarily due to TG lowering itself.
Omega-3 fatty acids consumption also improves triglycerides level and endothelial function, however, demonstrates inconsistent effects on inflammation, insulin resistance, and hemostasis.58)66) Although omega-3 fatty acids are bioactive compounds that play a significant role in cardiovascular and metabolic health and produce modest reductions in the rates of cardiovascular death in earlier randomized clinical trials, however, recent double-blind, randomized, clinical trials failed to show beneficial effects on cardiovascular events under modern guideline therapy.67)68) Further, omega-3 fatty acid or fish consumption was associated with a modestly higher incidence of type 2 diabetes in observational studies.69)70) However, this untoward effect seems to be neutral.
Taken together, fibrates might play an important role in the reduction of residual cardiovascular risk by favorable lipid profiles, endothelial function, inflammation and metabolic effects in patients with cardiovascular risks especially low HDL cholesterol and high triglycerides.3)11)58)62) However, a large-scaled clinical trial to investigate the effects of fibrate based on statin in patients with low HDL cholesterol and high TG level on the cardiovascular outcomes will be needed in the future. Though some studies reported no different effects of high dose omega-3 fatty acids except the reduction of triglycerides level,71) the role of omega-3 fatty acids, particularly a high dose, will be further elucidated with regard to the reduction of residual cardiovascular risk in the future. Three ongoing randomized controlled clinical trials (the Rischio and Prevenzione study),72) a Study of Cardiovascular Events in Diabetes (ASCEND, NCT00135226), the Vitamin D and Omega-3 Trial (VITAL, NCT01169259)73) in patients with low cardiovascular risk will further answer this question. In patients with high cardiovascular risk, reduction of cardiovascular events with EPA-intervention trial (REDUCE-IT, NCT 01492361) and outcomes study to assess residual risk reduction with epanova (STRENGTH, NCT02104817) are ongoing and will answer the effectiveness of high dose omega-3 fatty acids added on statin treatment for the cardiovascular outcomes.11)
Niacin, Bile acid binding resin and cholesteryl ester transfer protein
Niacin has a broad spectrum of lipid modifying activity which include HDL cholesterol raising and TG lowering effects.74) Although previous studies reported niacin had shown attenuation of atherosclerosis progression and reduction of non-fatal myocardial infarction and all-cause mortality,75)76) niacin has now been withdrawn following reports of safety issues in the HPS2-THRIVE trial.77) Bile acid binding resins are indicated for treatment of elevated plasma LDL cholesterol levels. Although hypertriglyceridemic patients with elevated LDL cholesterol levels are indicated the use of bile acid binding resins, most hypertriglyceridemia patients without elevated LDL cholesterol levels are contraindicated due to no effect or mild elevation of TG or an adverse effect on plasma TG concentration.78) Because CETP promotes exchange of cholesterol and TG between HDL and TRL, LDL and CETP inhibitors are expected to have anti-atherogenic effects by increasing the concentration of cholesterol in the protective HDL fraction, and decreasing proatherogenic LDLs or the cholesterol content of TRLs.79) However, recent large scaled randomized clinical trials such as ILLUMINATE and dal-OUTCOMES failed due to safety concerns or futility in major outcomes.80)81) It was explained that it was mainly due to adverse off-target effects or dysfunctional HDL. Therefore, currently CETP inhibitors are not recommended to management of hypertriglyceridemia. In addition, we need to wait the results of on-going clinical trials of CETP inhibitors including Randomized Evaluation of the Effects of Anacetrapib Through Lipid-modification (NCT01252953) and A Study of Evacetrapib in High-Risk Vascular Disease (ACCELERATE, NCT01687998).82)
Antisense inhibition of apolipoprotein C-III
ISIS 304801 is a second generation antisense inhibitor of APOC3 synthesis. This small chemically-modified oligonucleotide is delivered subcutaneously and is internalized in the liver where it inhibits the translation of APOC3 mRNA and promotes mRNA degradation through activation of RNase H.43) A randomized, double-blind, placebo controlled, dose ranging, phase 2 study revealed that treatment with ISIS 304801, at doses ranging from 100 to 300 mg, once weekly for 13 week, resulted in dose-dependent and prolonged decreases in plasma APOC3 levels when the drug was administered as a single agent.45) In addition, when it was administered as in combination with fibrates, treatment with ISIS 304801 resulted in reduction of APOC3 levels. Concordant reductions of 31.3 to 70.9% were observed in TG levels without any safety concerns. This study provides evidence for a causal relationship between APOC3 and TG metabolism. In addition, it supports the continued development of ISIS304801 for the treatment of patients who remain at risk for cardiovascular events and pancreatitis because of very high TG levels.
Angiopoietin-like proteins, Angiopoietin-like proteins 3 and Angiopoietin-like proteins 4
Like apoC-III, ANGPTL3 and ANGPTL4 are thought to inhibit LPL activity, leading to elevate plasma TG levels. Pharmacological inhibition of these ANGPTLs could reduce plasma TG by a mechanism similar to that of anti-APOC3-focused therapies and result in reduced CAD risk.43) However, recent evidence linking ANGPTL3 and ANGPTLs loss of function to CAD risk has been smaller or inconsistent.83)84)85)
Microsomal triglyceride protein inhibitor (lomitapide), diacylglycerol O acyltransferase 1 inhibitor, lipoprotein lipase gene replacement treatment
Lomitapide, an MTP inhibitor that interferes with apoB containing lipoprotein assembly in the apoB100 and apoB48 pathway, reduces both chylomicron and VLDL secretion.32) It is currently available for the management of homozygous familial hypercholesterolemia to treat a patient with extremely severe hypertriglyceridemia due to LPL deficiency.86) The limitation of lomitapide treatment is the possibility of developing steatohepatitis and fibrosis. The research for DGAT1 and LPL gene replacement treatment is still being tested.
Summary and Future Perspectives
Residual cardiovascular risk still exists even after optimal medical treatment including high dose statin treatment. After failure of HDL cholesterol raising treatment and genetic studies on HDL cholesterol, concern of the role of TRLs and remnant cholesterol regarding cardiovascular risk are increasing. Experimental, epidemiological and genetic evidence support the harmful effects of TRLs and remnant cholesterol. To reduce risk by hypertriglyceridemia, lifestyle intervention plays a key role. However, when hypertriglyceridemia or high levels of TRLs or non-HDL cholesterol are not corrected after lifestyle intervention with statin treatment, current available drugs such as fibrates are options for management of hypertriglyceridemia. Omega-3 fatty acids should be held until ongoing clinical trials are reported. In addition, new treatment options such as antisense inhibition of apolipoprotein C-III, ANGPTLs are being tested. The effectiveness of treatment of hypertriglyceridemia on cardiovascular outcomes will be answered in the future.
Conclusions
There is increasing evidence of the role of hypertriglyceridemia, TRLs and remnant cholesterol on cardiovascular outcomes. Effort for reducing levels of TG and TRLs including correction of secondary cause of hypertriglyceridemia and lifestyle intervention, fibrates, omega-3 fatty acids and new treatment options are encouraging. Randomized clinical trials of these treatments on beneficial cardiovascular outcomes are ongoing and will answer the exact role of treatment of TG and TRLs in the future.



 XML Download
XML Download