

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Constrictive pericarditis occurs when cardiac filling is excessively constrained by the pericardium. Although it is rare in comparison with other causes of congestive heart failure, constrictive pericarditis is an important diagnosis because of it is curable. Constrictive pericarditis has multiple causes. In some cases, bullets are associated with pericarditis, causing rhythm and conduction abnormalities. Constrictive pericarditis induced by bullets has been reported. In this case report, we present a patient who was shot in the Korean War and had a bullet inside the pericardium and had pericarditis and atrial flutter after an asymptomatic period of over 60 years.
Case
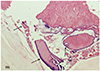
A 69-year-old man visited our hospital for palpitation and dyspnea on exertion. The symptoms began four months prior to his visit to the hospital. On physical examination, a rapid heartbeat and friction rub were audible, and a 6-cm linear scar was observed on the right upper chest. Edema of both lower extremities was observed. At the age of 6 in 1950, he was wounded in the chest during a shooting spree by North Korean soldiers during the Korean War. However, at that time he could not visit a hospital and was treated with folk remedies. On the chest X-ray, a bullet adjacent to the right cardiac border and bilateral pleural effusion was noted (Fig. 1). On electrocardiography, he had typical atrial flutter with 2-to-1 atrioventricular conduction, and his heart rate was 150 bpm (Fig. 2). An axial computed tomographic image (Fig. 3A) showed that the bullet was likely located in the right atrium. Thickening of the pericardium was also observed. A long axis reformatted image (Fig. 3B) and a three-dimensional volume-rendered image (Fig. 3C) confirmed that the bullet was located in the epicardial fat and abutted the right atrium at an acute angle. Transthoracic echocardiography during the atrial flutter and sinus rhythm revealed bi-atrial enlargement, thickened pericardium, septal bouncing motion, and significant respiratory variations of the mitral inflow velocity, which were compatible with constrictive pericarditis (Fig. 4). The E/A and E/e' ratios were 4.4 and 8, respectively. The septal e' was higher than the lateral e' (12 cm/sec and 10 cm/sec, respectively). To rule out lead poisoning from the bullet, the patient's blood lead level was checked and lead was undetectable. Atrial flutter and constrictive pericarditis were the suspected causes of the palpitation and dyspnea on exertion. An electrophysiological study confirmed that the atrial flutter was cavotricuspid isthmus-dependent: during the electrophysiological study, fluoroscopy showed that the bullet moved primarily with respiratory movements and partially with heart-beating movements. Moreover, pericardial calcification was also observed adjacent to the coronary sinus. Radiofrequency catheter ablation for ty-pical atrial flutters was performed by a bidirectional conduction block of the cavotricuspid isthmus. One week after radiofrequency catheter ablation, surgical extraction of the bullet and pericardiectomy were performed. In the surgical field, the pericardium was th-ickened and the bullet was severely adhered to the adjacent epicardial tissue (Fig. 5). There were scattered substances around the bullet, which were presumed to be gunpowder. Due to the gunpowder, the pericardium was thickened and stiffened. The rusted bullet was extracted 63 years after the initial gunshot wound. The pathology of the adjacent epicardial tissue showed dystrophic calcification (Fig. 6). After surgery, the patient recovered without complications and there was no echocardiographic evidence of constrictive physiology.
Discussion
Constrictive pericarditis is an uncommon post-inflammatory disorder characterized by a variably thickened, fibrotic, and frequently calcified, pericardium. The resulting distinctive pathophysiologic characteristics produce signs and symptoms of predominantly systemic venous congestion.1) The etiology of constriction can vary, including prior cardiac surgery (most common in the USA), viral pericarditis, no known cause (idiopathic), prior chest radiotherapy, con-nective tissue disease, human immunodeficiency virus infection, and tuberculosis.2) Although foreign bodies are not the common cause of constrictive pericarditis, foreign bodies can induce constrictive pericarditis.3)4) Cardiac injuries can occur from various agents, and in many cases of constrictive pericarditis due to the injury, the agents include needles, knives, and other foreign bodies.5) In 1956, Dressler6) showed that patients with post-cardiac injuries subsequently developed pericarditis as a result of an autoimmune reaction, which is the principle pathophysiological manner of trauma-induced pericarditis. Several cases regarding pericarditis or pericardial effusion induced by gunshot have been reported.7)8)9)
Three factors (acute bacterial pericarditis, foreign body reaction, and hemopericardium) can contribute to the development of chronic constrictive pericarditis in patients with intra-cardiac foreign bodies. Contaminated foreign bodies can cause pericarditis long after entering the pericardial space. One case reported constrictive pericarditis developing 45 years after a gunshot wound.7) In a series of 143 patients with surgically confirmed constrictive pericarditis, 22 percent had atrial fibrillation.10)
The patient was extremely fortunate to survive the initial gunshot wound; the bullet stopped just before reaching his heart, between the right atrium and the superior vena cava. In other cases, the bullet or foreign body is retained without surgery in asymptomatic and healthy patients. But in this case, constrictive pericarditis and atrial flutter occurred after an asymptomatic period of 63 years. The long-term presence of a bullet in the pericardium or epicardium can be a rare cause of constrictive pericarditis, because the bullet and gunpowder can induce chronic inflammation. Atrial flutter can accompany constrictive pericarditis due to the atrial enlargement resulting from the constrictive physiology.
Retained cardiac bullets without any specific signs or symptoms of a cardiovascular problem can be treated conservatively. In contrast, there is a report of a case where pericardial irritation and effusion may develop up to 2 years after the injury.11) In this case, pericarditis occurred after very long asymptomatic period from cardiac injuries resulting from the bullet. In chronic constrictive pericarditis, pericardiectomy is the only definitive treatment option for patients with chronic constrictive pericarditis. In this case, after the long asymptomatic period, constrictive pericarditis was induced.
Although constrictive pericarditis induced by a bullet is rare, the long-term presence of a bullet can be presumed to be a cause of constrictive pericarditis.





 XML Download
XML Download