

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Platypnea-orthodeoxia syndrome (P-Os) is a rare cause of dyspnea and is characterized by dyspnea while in an upright position.1)2)3) Platypnea means that dyspnea is induced by an upright posture and is relieved by adopting a recumbent position. And orthodeoxia means an arterial desaturation resulting from orthostatic conditions.3)4) Although the exact mechanisms are not yet known, possible causes include three categories; intracardiac shunting, pulmonary arteriovenous shunts or ventilation/perfusion mismatch in the lungs.5)6) Patent foramen ovale (PFO) is the most common cause among intracardiac shunt groups, followed by atrial septal defect (ASD) and fenestrated atrial septal aneurysm.6) Herein we report a case of a patient with P-Os caused by ASD with normal right atrial pressure. To the best of our knowledge, this is the first case in Korea of successful treatment with a device closure in an ASD patient presenting with P-Os.
Case
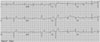
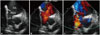
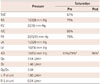
A 29-year-old female was referred to our institute with symptomatic hypoxemia with one-week duration in April 2013. Her dyspnea was aggravated while sitting or standing and relieved while in supine position. She had experienced intermittent dyspnea on exertion since school age, but she had not been evaluated until this visit. She had been suffering from intermittent migraines with visual aura since 1998 and had been treated with intermittent analgesics since then. The brain magnetic resonance imaging taken in 2008 showed normal results. She had neither a history of hypertension, diabetes mellitus or pulmonary disease nor a family history of pulmonary or cardiovascular disease. The pulse oximetry showed a saturation of 92% in a supine position, but this declined to 77% within one minute after standing indoors at atmospheric pressure. Recovery of the hypoxemia was not sufficient, as 94% was reached in a supine position and 82% was reached within one minute after standing despite supplemental oxygen therapy (100% oxygen, delivered via facemask). Her blood pressure was 107/69 mm Hg, her pulse rate was 72 beats per minute and her body temperature was 36.5℃. A grade III systolic cardiac murmur was heard on the left upper sternal border, the electrocardiogram (ECG) showed a sinus rhythm with premature ventricular complexes (PVC) and RSr' pattern in V 1 (Fig. 1). The lung sound was clear and chest X-ray (Fig. 2) and spirometer were both normal, so there was no apparent pulmonary disease that could explain the dyspnea. A transthoracic echocardiography (TTE) showed an 8-mm-sized ASD with a right-side volume overload and a left-to-right shunt through ASD. There was a trivial tricuspid regurgitation with peak pressure gradient of 22 mm Hg. Although the TTE image was interrupted by a poor echo window, the coronary arteries showed a normal pattern. The contrast-enhanced computed tomography (CT) showed no pulmonary thromboembolism, pulmonary arteriovenous fistula or lung parenchymal disease. A 12-mm sized ASD and mild kyphoscoliosis were evident in the CT. The ASD shown on TTE and the heart CT could not explain the patient's dyspnea, so a cardiac catheterization was performed to evaluate the presence of pulmonary hypertension or a right-to-left shunt lesion, which would be masked on TTE or CT. The cardiac catheterization showed a normal pulmonary artery pressure and a normal right atrial pressure (Table 1). A 34-mm-sized ASD was seen by the intracardiac echocardiogram. The size of the ASD had been underestimated, possibly due to the poor echo window by TEE and transient bidirectional shunt by CT. During catheterization, a Valsalva maneuver was performed that showed a bidirectional shunt via ASD (Fig. 3) and the patients' arterial oxygen saturation decreased from 93% while in supine position to 79% while at a 15° sitting position. Finally, she was diagnosed as suffering from ASD with P-Os. An ASD device closure with an Amplatzer® septal occluder (36 mm, St. Jude Medical, Golden Valley, MN, USA) was successfully done under intracardiac echocardiogram guidance (Fig. 4), which resulted in the disappearance of both platypnea and orthodeoxia immediately after the procedure. The arterial oxygen saturation after closure was also improved to 96%. The patient has been free of symptoms for one year of follow-up and a recent TTE performed in April 2014 showed normal findings, including no residual ASD shunt.
A Holter monitoring was performed before catheterization and revealed 22% of PVCs. The patient was treated with oral propranolol, but it was discontinued soon due to symptomatic bradycardia. She has been free from symptoms such as palpitation for one year and the latest ECG performed in June 2014 showed a normal sinus rhythm. During her hospitalization, the patient complained of migraine headaches with visual aura three times a week and was treated with topiramate 25 mg twice daily. The brain magnetic resonance imaging and the angiography performed to check for cryptogenic stroke related to migraines, which would be due to a paradoxical embolism, showed no abnormalities in the brain parenchyma or intracranial and neck vessels. The migraine headache disappeared by three months after the ASD device closure and did not recur for one year, despite stopping taking topiramate six months after the ASD device closure.
Discussion
Platypnea-orthodeoxia syndrome is a rare clinical syndrome that is characterized by dyspnea while in an upright position. Three causes are possible: intracardiac shunts, pulmonary arteriovenous shunts or ventilation/perfusion mismatches in the lungs. Pulmonary arteriovenous shunts are usually located in the lung bases; increased flow in the lung base while in an upright position may increase the shunt, causing aggravated dyspnea and hypoxemia. A ventilation/perfusion mismatch would explain the mechanism of P-Os in some groups: hepatopulmonary syndrome, amiodarone toxicity, autonomic dysfunction and lung parenchymal disease such as emphysema.6) A failure to accommodate the gravitational blood flow changes due to an impaired pulmonary vascular tone while in an upright position, especially in the basal alveoli, is a possible mechanism in the former three groups. When standing upright, the right ventricular preload decreases, resulting in a decreased output to the pulmonary arteries, so that the alveolar pressures exceed the arterial and venous pressures.6) Moreover, a decreased blood flow at the apex due to gravity makes apical areas act as dead space while in an upright position. This phenomenon would explain the mechanism of P-Os in a lung parenchymal disease. Intracardiac P-Os are associated with the interatrial communication: PFO is most common, followed by ASD secundum, atrial septal aneurysm7) and ASD ostium primum. In this situation, the right-to-left shunt can be caused when the right side pressure is elevated or when the heart-lung anatomy is distorted and the venous blood is redirected towards the interatrial communication. An elevated right atrial pressure is usually linked to a decreased right ventricular compliance, but is sometimes related with pulmonary arterial hypertension. This etiology group includes pulmonary embolism,8) constrictive pericarditis,9) pericardial effusion,10) and right ventricular myocardial infarction.11) Anatomical distortions include aortic dilatation, aortic elongation12) and persistent Eustachian valve. Other causes of anatomical distortion are right pneumonectomy, kyphoscoliosis4) and phrenic palsy. The present patient was diagnosed as having P-Os caused by ASD and being affected by kyphoscoliosis. She was successfully treated by transcatheter device closure with an Amplatzer® septal occluder (St. Jude Medical), which resulted in the resolution of both platypnea and orthodeoxia immediately after the procedure. Interestingly, she had been suffering from migraine headaches with visual aura for several years, which then disappeared three months after device closure. There is a well-known relationship between PFO and migraines and that the treatment of PFO would reduce or eliminate migraine headache is estabilished.13) The relationship between ASD and migraine was not well established. However, according to Mortelmans et al.,14) a percutaneous ASD closure was not related to a decrease in the prevalence of migraine. Nevertheless, in the subgroup of patients who suffered from typical migraines before ASD closure, the frequency of migraine attacks decreased significantly. Luermans et al.'s15) findings supported this relationship in a prospective study. P-Os is a rare and complex clinical disease entity that must be considered in the differential diagnosis of unexplained postural hypoxemia, and it is important to pay attention to the pattern of dyspnea. Many patients may not be correctly diagnosed due to routine examination with an ECG, chest roentgenogram or even with TTE, as in our case.
The diagnosis of cardiac P-Os consists of the demonstration of the presence of a right-to-left shunt and the documentation of an orthodeoxia with either pulse oximetry or blood gas analysis. A contrast TTE may demonstrate this phenomenon, but a contrast transesophageal echocardiography in both a supine and upright position is the preferable choice for diagnosis. Recently, a percutaneous device closure has been considered as a treatment of choice for cardiac P-Os, since this approach has proven to be safe, reliable and effective.16) Before considering a percutaneous closure, a cardiac catheterization is required with a complete evaluation of oxygen saturation and pressure. As in our case, the size difference of ASD should be evaluated during Valsalvar maneuver and it is crucial to select the proper sized device in the transcatheter closure of ASD.
In conclusion, P-Os should be considered in the differential diagnosis in patients with unexplained hypoxemia. Herein, we present the first Korean case of transcatheter treatment of ASD presented with platypnea and orthodeoxia, and discuss the pattern of dyspnea, diagnostic approach and the mechanisms of intracardiac P-Os. Lastly, this case highlights the importance of a complete evaluation with cardiac catheterization and careful percutaneous closure.


 XML Download
XML Download