

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Immunoglobulin G4-related disease (IgG4-RD) an autoimmune disease characterized lymphoplasmacytic tissue infiltration with a predominance of IgG4-positive plasma cells. Although IgG4-RD can affect any organ, the majority of cases have been reported involving the biliary tract or pancreas. Only two cases of constrictive pericarditis caused by IgG4-RD have been reported. This is a first case report of constrictive pericarditis caused by IgG4-RD in Korea.
Case
A 58-year-old man visited our outpatient clinic with a seven-day history of dyspnea. He suffered from progressive dyspnea, orthopnea, and general weakness. In 2009, he had undergone a bilateral thyroidectomy with modified radical neck dissection at another hospital due papillary thyroid cancer. He had been taking 100 micrograms (mcg) of levothyroxine once daily for three years.
During the pre-operative evaluation of his thyroid cancer at the other hospital, a small to moderate amount of pericardial effusion was noted on the transthoracic echocardiogram (TTE). Because the patient did not have any symptoms of pericardial effusion, the cardiologist recommended follow-up TTEs every six months.
The initial physical exam on the first day of hospitalization revealed a blood pressure of 130/60 mm Hg, pulse rate of 92 beats per minute, respiratory rate of 18 breaths per minute, body temperature of 37.0℃, and oxygen saturation of 96% while the patient was breathing ambient air. Jugular venous distension was observed while the patient was sitting. There was no bruit or murmur. Bilateral pretibial edema was observed, and decreased lung sounds were heard at the bilateral lower lung fields.
Findings of laboratory tests on the first day of hospitalization indicated a normal complete blood count, as well as normal levels of blood urea nitrogen, creatinine, total protein, albumin, aspartate aminotransferase, alanine aminotransferase, and electrolytes. The blood levels of triiodothyronine, thyroxine, and thyroid-stimulating hormone were within normal limits (0.69 ng/mL, 1.51 ng/dL, and 1.93 µIU/mL, respectively). The levels of serum anti-nuclear antibody, anti-deoxyribonucleic acid enzyme linked immunosorbent assay, anti-Smith antibody, P-antinuclear and antineutrophil cytoplasmic autoantibodies (ANCA), C-ANCA, anti-Scl 70, and lupus anticoagulant were negative. The patient's blood level of C-reactive protein was 21.5 mg/L, erythrocyte sedimentation rate was 33 mm/hr, complement 3 (C3)/C4 was 131.5/31.09 mg/dL, and lactate dehydrogenase (LDH) was 213 IU/L, which were all within normal levels. Serum levels of IgG (1473 mg/dL) and subclass IgG4 (1503.9 mg/L) were elevated. Three sputum acid-fast bacillus (AFB) smears and cultures were negative, and interferon gamma (IFN-γ) release assay tests for tuberculosis were also negative (Nil: 0.06, TB Ag: 0.11, Mitogen: 14.87).
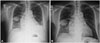
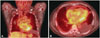
We detected bilateral pleural effusion with loculation along the right minor fissure with moderate cardiomegaly on the patient's chest radiograph (Fig. 1A). On the TTE from the first day of hospitalization, we observed constrictive physiology with a small amount of organized pericardial effusion (Fig. 2A). Pericardial effusion with mild fluorodeoxyglucose uptake was observed on positron emission tomography-computed tomography, likely due to inflammatory processes (Fig. 3). Bilateral pleural effusion was also observed.
Furosemide (20 mg twice daily) and spirolactone (12.5 mg twice daily) were prescribed to control the patient's dyspnea and pretibial pitting edema, and other laboratory studies were conducted to detect the cause of the constrictive pericarditis.
To diagnose and treat the patient's idiopathic constrictive pericarditis, we performed a pericardial effusion drainage and biopsy on HOD 3. On the pericardial effusion study, many (uncountable) red blood cells and white blood cells were observed. The test results showed 4 g/dL of protein, 2.5 g/dL of albumin, 123 IU/L of LDH, 142 mg/dL of glucose, and 43.7 IU/L of adensine deaminase. Mycobacterium tuberculosis complex polymerase chain reaction (PCR) of the pericardial fluid, AFB smears, and culture were all negative. Histopathology of the pericardial biopsy revealed mild chronic inflammatory cell infiltration with fibrosis, but there was no evidence of IgG4 cell infiltration.
After drainage of the pericardial effusion, we observed a temporary improvement of dyspnea, but it was aggravated on HOD 7. Therefore, we decided to perform a pericardiectomy on HOD 11. Histopathology findings of the pericardiectomy revealed a diffuse coating of fibrinous exudate with mild lymphocytic infiltration with IgG4-positive cells (30/HPF, IgG4/IgG ratio: 5%) (Fig. 4). Therefore, we diagnosed pericarditis caused by IgG4-RD, and prednisolone (40 mg) was initiated to treat the persistent mild dyspnea after the pericardiectomy. As the patient's symptoms disappeared, he was discharged and during follow-up, we observed resolution of the pericardial effusion and bilateral pleural effusion on the chest X-ray and TTE (Figs. 1B and 2B).
Discussion
Immunoglobulin G4-related disease is an autoimmune disease that may involve any organ, characterized by a lymphoplasmacytic infiltrate enriched in IgG4-positive plasma cells, and variable degrees of fibrosis.1) Target organ biopsy and histopathology are the most important diagnostic methods. For most tissues, the diagnosis is made from 30 to 50 IgG4-positive cells/HPF.2) Sometimes serum IgG4 levels are elevated in IgG4-RD, but serum IgG4 concentrations are neither sufficiently sensitive nor specific for diagnosis of this disease.3) The natural course of IgG4-RD is not well-defined. Generally, it is effective to treat IgG4-RD with moderate to high doses of steroids. Some previous reports have demonstrated that IgG4-RD spontaneously regressed without treatment.4) However, when vital organs are involved, aggressive treatment is needed because IgG4-RD can lead to serious organ dysfunction and failure.5)
Constrictive pericarditis occurs in approximately 2-3% of cases after pericarditis,6) and 40-50% of cases are idiopathic in origin.7) While the most common cause is thought to be viral infection, the association of viral infection with IgG4-RD is a source of much debate. There is a lack of consensus regarding the incidence, etiology, and treatment of IgG4-RD. Several case reports have been published worldwide, including a case of a 78-year-old male with constrictive pericarditis confirmed to have IgG4-RD after pericardiectomy,8) and a second case of a 29-year-old female with lung en-trapment and constrictive pericarditis caused by IgG4-RD.9) After pericardiectomy, symptoms disappeared in the first patient and no further treatment was necessary. The second patient required prednisolone (40 mg/day) for 2 weeks with gradual tapering.
The patient's adenosine deaminase (ADA) level was 43 IU/L, and therefore, within the lower limit of diagnosis for tuberculous pericarditis (TB pericarditis). However, he did not have any clinical symptoms of TB pericarditis such as fever, night sweating, or weight loss. Moreover, TB PCR, AFB smear, and IFN-γ release assay testing for tuberculosis were all negative. Therefore, we ruled out the possibility of TB pericarditis in the patient.
As tuberculosis is endemic in South Korea, and TB pericarditis is the second most common cause of constrictive pericarditis after idiopathic pericarditis,9) IgG4-RD can easily be misdiagnosed as TB pericarditis since pericardial fluid ADA levels may be increased over 40 IU/L. Consequently, this can lead to a prolonged use of TB medication.10)
The first pericardial biopsy of the patient did not reveal any IgG4-positive cells. However, the pericardiectomy histopathology was positive for IgG4-positive cells. We hypothesize that focal infiltration of IgG4 cells in the pericardium may have resulted in the initial false negative result.


 XML Download
XML Download