

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Previous studies have shown that the introduction of drug-eluting stents along with advances in peri- and post-procedural adjunctive pharmacotherapies has improved the outcomes of percutaneous coronary intervention (PCI) for coronary artery stenosis,1) and these advances have rendered PCI with stenting a viable alternative to coronary artery bypass graft (CABG) surgery. Standard guidelines, however, still do not recommend PCI except for patients with unprotected left main coronary artery stenosis who are at high surgical risk or in emergency clinical situations, such as bailout procedures or for treatment of acute myocardial infarction (MI). These recommendations have largely been based on the recent findings that CABG, as compared with PCI, resulted in lower rates of major adverse cardiac or cerebrovascular events.2)3)4)
Among the currently available algorithms, the Synergy between PCI with Taxus and Cardiac Surgery (SYNTAX) score, is one the most extensively studied scores. Although the SYNTAX score was initially formulated to comprehensively represent angiographic complexity, which is considered an important determinant of outcomes after PCI or CABG for treatment of multivessel coronary disease,5)6) it is also able to predict major adverse cardiac events (MACE) after percutaneous revascularization in patients with multivessel coronary artery disease (CAD)3)5)7)8)9)10)11)12) or left main disease.13)14)
The SYNTAX score was pioneered as an anatomical-based risk score to aid in the decision-making process; the lack of clinical variables in this score has, however, been its main limitation.15)16) A significant improvement in the prediction of cardiac mortality observed after the inclusion of EuroSCORE in a SYNTAX score-based model indicated that clinical and angiographic information are both important for assessing individual risk of patients undergoing left main PCI.17)
New insights into inflammation in atherosclerosis have practical clinical applications in risk stratification.18)19)20) Pentraxin 3 (PTX3) was initially described as an early marker for primary local activation of innate immunity and inflammatory response.21)22)23) Because PTX3 release is likely to be a specific response to vascular damage, PTX3 levels may provide more explicit information on development and progression of atherosclerosis than nonspecific markers like C-reactive protein.24)25)26)27) Currently available evidences suggest a potentially important regulatory role for PTX3 in the modulation of the immune-inflammatory response associated with atherosclerosis and ischemic cardiovascular injury. Whether part of this protective effect could be mediated through local up-regulation of PTX3 in vascular endothelial cells remains to be clarified. We have recently shown that coronary sinus as well as systemic arterial PTX3 levels can improve the estimation of the pretest probability of presence of angiographically-detected CAD.28)
Our previous findings were based on the presence or absence of significant coronary artery stenosis. To the best of our knowledge, none of the studies have investigated whether PTX3 can predict the angiographic complexity of CAD among patients with ischemic heart disease. In the current study, we primarily aimed to examine the hypothesis that increased levels of PTX3 can predict angiographic complexity of coronary artery stenosis as measured by the SYNTAX score.
Subjects and Methods
Study population
Among the patients who were referred to two large referral cardiac hospitals (the Golestan Heart Hospital, Ahvaz, Iran and Modarres Heart Hospital, Tehran, Iran), we consecutively recruited 500 patients whose ischemic heart disease was diagnosed first. The patients were assigned to medical therapy (251), PCI (197), or CABG (52) based on the clinical judgment of their cardiologists who were blinded to the results of the SYNTAX score. Data on age, sex, smoking, hypertension, diabetes, and cholesterol levels, as well as on echocardiographically determined ejection fraction were obtained from patients' hospital records.
Ethics
We certified that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research. Informed written consent was obtained from all of the participants and the Ethics Committee of Ahvaz Jondishapur University of Medical Sciences approved this study. The study protocol conformed to the ethical guidelines of the 2008 Declaration of Helsinki.
Laboratory measurements
Blood samples drawn from the femoral artery were centrifuged immediately and stored at -70℃, and then used for measurement of femoral artery PTX3 and high sensitivity C-reactive protein (hs-CRP) concentrations. Analyses were performed using Cusabio kits (Cusabio Biotech, Wuhan, Hubei Province, China) for hs-CRP. Plasma PTX3 concentration was measured by using a commercially available Human PTX3 enzyme-linked immunosorbent assay kit (CUSABIO BIOTECH CO., Ltd., Wuhan, China). Details of the assay have been described elsewhere.29) Briefly, the microtiter plates provided in the kit were pre-coated with an antibody specific to PTX3. Standards or samples were then added to the appropriate microtiter plate wells with a biotin-conjugated antibody preparation specific for PTX3, and Avidin conjugated to Horseradish Peroxidase was added to each micro-plate well and incubated. Then, the TMB (3,3',5,5' tetramethylbenzidine) substrate solution was added to each well. The enzyme-substrate reaction was terminated by the addition of sulphuric acid solution and the color change was measured spectrophotometrically at a wavelength of 450±2 nm. A Selectra 2 auto-analyzer (Vital Scientific, Spankeren, Netherlands) was used to analyze the samples.
Diagnostic angiographic examinations
Diagnostic angiography was performed in all of the participants within 24 hours of the diagnosis of MI or unstable angina and in participants with chronic stable angina who had at least one positive noninvasive test result {e.g., positive stress tolerance treadmill electrocardiogram (ECG)}. Angiographies were done by Judkins right and left catheters, all through femoral artery and by Germany's Siemens Axiom Artis DFC ZEE floor-mounted device. Interpretation of angiographs was performed by two expert cardiologists who were blinded to the blood tests results (femoral artery PTX3 levels). The quantification analysis of obstructions after calibration of the catheter was performed by moving the cursor from the proximal through the distal of each vessel for revealing the length and severity of the obstruction. All three coronary arteries (right CA, left CA, and lateral circumflex). Quantitative coronary angiography was performed in biplane views. The measurement of SYNTAX score was retrospectively performed on baseline angiograms. The SYNTAX score was calculated using Calculator 2.11 (available at: http://www.syntaxscore.com). The SYNTAX score was calculated in accordance with the algorithm, which is the sequential morphological evaluation of dominance; number of lesions; segments involved per lesion; and presence of total occlusion, trifurcation, bifurcation, aorto-ostial lesion, severe tortuosity, length >20 mm, heavy calcification, thrombus, and diffuse/small vessels in lesions for each patient.6) The score was independently analyzed by the cardiologist. To decrease interobserver variation, the scores were measured by the same cardiologist. A low SYNTAX score was defined as values <23 since the 3-year SYNTAX results suggest that CABG remains the standard of care for patients with complex disease (intermediate i.e., 23-33 or high SYNTAX scores i.e., >33) and that PCI may be an acceptable alternative revascularization method to CABG when treating patients with less complex (lower SYNTAX Score) disease.13)18) As such, we ascertained complex coronary artery stenosis among participants with a SYNTAX score ≥23.
Blood sampling for determining pentraxin 3 and high sensitivity C-reactive protein concentrations
Before angiography, a blood sample was taken from the femoral artery. Whole blood was immediately collected into a tube containing ethylenediaminetetraacetate.
Definitions of terms
A specific outcome was assigned for each event according to International Statistical Classification of Diseases and Related Health Problems criteria (10th Revision), and the American Heart Association classification for cardiovascular events.21)22)23) CAD included cases of definite MI diagnosed by ECG and biomarkers, probable MI (positive ECG findings plus cardiac symptoms or signs and biomarkers showing negative or equivocal results), unstable angina pectoris (new cardiac symptoms or changing symptom patterns and positive ECG findings with normal biomarkers), and angiographically proven MI. The following criteria were used to make the diagnosis of an acute, evolving or recent MI: time-dependent changes in troponin and MB fraction of creatine kinase (CK-MB) activity {typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis} with at least one of the following:
Statistical analysis
Descriptive analysis
Descriptive data have been presented as mean (SD) or median (IQR) for continuous variables with normal and non-normal distribution, respectively. Categorically distributed variables have been described in terms of frequency (n, %).
Primary associations
The statistical significance of the trends in risk factors across increasing quartiles of the SYNTAX score was examined either by logistic regression models or Kruskal-Wallis test. We examined the predictive ability of the candidate risk factors for complex coronary artery stenosis by implementing a special regression modeling approach. Owing to the high prevalence rate of complex coronary artery stenosis in the study population, the odds ratios obtained from the logistic regression model would be excessively large.27) Therefore, to approximate the relative risk of having complex coronary artery stenosis with increasing levels of CAD risk factors, we used the Cox proportional hazard regression model using the robust estimator of variance. We set the time at risk to a constant value (i.e., 1) for all of the participants.22) When a constant risk period is assigned to everyone in the cohort, the hazard rate ratio estimated by Cox regression equals the cumulative incidence ratio in longitudinal studies, or the prevalence ratio in cross-sectional studies.23) We used several criteria to compare the overall diagnostic values of alternative models; Goodness-of-fit, discrimination, calibration, index of determination or explained variation, added predictive ability, and nonlinear associations (Appendix in the online-only supplement).
The statistical significance level was set at a two-tailed type I error of 0.05. Instead of adjusting for multiplicity of inference we reported pure p so that the readers can decide on the significance of the findings. All statistical analyses were performed using STATA version 12 (STATA, College Station, TX, USA).
Results
Median (IQR) age of the participants was 54 years14) with 50.6% of subjects being males. Baseline characteristics of the participants by quartiles of the SYNTAX score are presented in Table 1. Median SYNTAX score was 12.18) Median systemic arterial PTX3 was 0.24 (0.13) ng · dL-1. Median age, total cholesterol levels, and systemic arterial levels of PTX3 were increased across increasing quartiles of the SYNTAX score in a stepwise fashion. Ejection fraction was decreased across increasing quartiles of the SYNTAX score.
The clinical judgment of the cardiologists was near-perfectly concordant with the SYNTAX score (Fig. 1). Mean (99% CIs) SYNTAX scores were 5.8 (5.1-6.6), 18.4 (17.1-19.8), and 33.2 (32.8-33.6) in the patients assigned to medical therapy, PCI, and CABG, respectively.
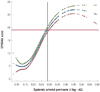
The AROC (95% CIs) for discriminating patients with and without complex coronary artery stenosis (SYNTAX score ≥23) was 0.920 (0.895-0.946) for systemic arterial levels of PTX3. As shown in Fig. 2, systemic arterial levels of PTX3 were associated with SYNTAX scores in a curvilinear fashion. The association curve was hyperbolic with three critical values. The minimum value of the SYNTAX score corresponded to the systemic arterial PTX3 level of 0.15 ng · dL-1, the maximum value to 0.45 ng · dL-1, and the point of inflection to 0.29 ng · dL-1. When we examined the diagnostic value of the systemic arterial PTX3 at the cutpoint of 0.29 ng · dL-1, which corresponded to the SYNTAX score of 23, we observed that the sensitivity was 0.66 (95% CIs 0.57-0.74), the specificity was 0.94 (95% CIs 0.91-0.96), the positive predictive value was 0.79 (95% CIs 0.70-0.87), and the negative predictive value was 0.89 (95% CIs 0.85-0.92).
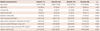
As shown in Table 2, the predictive performance of the basic model incorporating traditional CAD risk factors was significantly improved when systemic arterial PTX3 levels were also introduced into the basic model. When we used cutpoints of 25 and 50% to define risk categories, systemic arterial PTX3 helped to reclassify 0.35% (95% CIs: 0.27-0.42) of the patients into a more appropriate category.
The systemic arterial levels of hs-CRP were not found to be associated with the SYNTAX score.
Discussion
We investigated the predictive ability of the systemic arterial levels of PTX3 for the angiographic complexity of CAD as measured by the SYNTAX score, and we observed that systemic arterial levels of PTX3 were associated with the SYNTAX score in a curvilinear fashion. The discriminatory power of systemic arterial levels of PTX3 for a high SYNTAX score was outstanding.
Herein, we have extended our previous finding of the predictability of PTX3 for the presence/absence of coronary artery stenosis to the angiographic complexity of coronary artery stenosis. This finding provides a basis upon which longitudinal studies can be designed and performed to evaluate how PTX3, as a stand-alone or in combination with the SYNTAX score, predicts post-MI adverse effects. Our observations will be practically appealing when seen in light of the fact that when using the SYNTAX score, physicians are still challenged with a labor-intensive calculation and conflicting results from validation studies.26) When we examined the diagnostic value of the systemic arterial PTX3 at the cutpoint of 0.29 ng · dL1, which corresponded to the SYNTAX score of 23, we observed that the sensitivity, specificity, and positive and negative predictive values were 0.66, 0.94, 0.79, and 0.89, respectively. These findings provide clear evidence that before information from angiographic examinations is available, if the PTX3 cutpoint of 0.29 ng · dL-1 is applied, 89% of the patients with a low PTX3 level will not need CABG as indicated by the high SYNTAX score; meanwhile only 6% of the patients with a low SYNTAX score had a high PTX3 level. This indicates that the systemic arterial PTX3 level of 0.29 ng · dL-1 was highly specific for diagnosing complex coronary artery stenosis.
The SYNTAX score is increasingly attracting attention as an anatomically-based tool that helps cardiologists to objectively determine the complexity of CAD and to guide in decision-making between CABG surgery and PCI. External validity of the clinical usefulness of the SYNTAX score for identifying higher-risk patients and for aiding in decision-making between CABG and PCI has been confirmed by numerous studies and in a broad range of patients.27) Experienced angiographic core laboratory technicians have been reported to quickly achieve highly reproducible SYNTAX score measurements. In contrast, agreement among the interventional cardiologists after the basic tutorial has been reported to be initially poor but to improve considerably after further training with the angiographic core laboratory technicians. These findings have important implications for adoption of the SYNTAX score methodology in routine practice and future clinical trials.26)
We have previously quantified the improvement in estimating pretest probability of CAD offered by systemic arterial PTX3 over the traditional CAD risk factors. Systemic arterial PTX3 helped to more accurately reclassify patients with intermediate-risk chronic stable angina. After allowing for the effect of systemic arterial PTX3, high density lipoprotein-cholesterol (HDL-C) did no longer confer any protective effect, suggesting that the atheroprotective effect of HDL-C was mediated by PTX3. This finding shows that PTX3 might be a marker of CAD, the level of which increases to regulate the inflammation.28) Most recently it has been shown that among patients with chronic stable angina, PTX3 is more tightly associated with the complexity and severity of CAD than hs-CRP and it was found to be an independent predictor for high SYNTAX score.27)
Experienced cardiologists' gestalt is useful in estimating the pretest probability for adverse outcomes and is complementary to diagnostic testing, such as stress tolerance treadmill ECG. However, it is unclear whether the recently developed prediction rule, using explicit features of angiographic examination, is comparable with cardiologists' gestalt. If it is so, the SYNTAX score would be powerful tool because it could be used by less-experienced cardiologists to simplify the prognostication of MACEs. The important finding of our study was the near perfect concordance between the decisions made by the cardiologists based on their clinical judgment and the SYNTAX score. The clinical judgment of experienced cardiologists and the SYNTAX score that can be used by the cardiologists having varying experience showed similar accuracy in discriminating patients who need CABG from those who need PCI.
Strengths and limitations
The strengths of our study lie in its design, setting, and appropriate statistical approach. We recruited patients who were assigned to varying treatment methods including PCI and CABG. Our findings, however, need to be interpreted in light of its limitations. Due to the cross-sectional nature of the current study we were not able to compare the prognostic significance of PTX3 with that of the SYNTAX score for MACEs. We did not have data on PTX3 concentration in the vein, which might be more easily available. However, we have previously shown that systemic arterial levels of PTX3 have a good correlation with coronary sinus levels of PTX3, which can represent the venous blood concentration of PTX3.
If PTX3 is confirmed to be predictive of MACEs by prospective studies in the future, it can supplement the prognostic power of SYNTAX score in predicting post-MI adverse outcomes.
In conclusion, we investigated the predictive ability of the systemic arterial levels of PTX3 for the angiographic complexity of CAD as measured by the SYNTAX score and observed that the systemic arterial levels of PTX3 were associated with the SYNTAX score in an almost hyperbolic fashion. The discriminatory power of the systemic arterial levels of PTX3 for high SYNTAX score was excellent. The systemic arterial PTX3 level of 0.29 ng · dL-1 was highly specific for diagnosing complex coronary artery stenosis.


 XML Download
XML Download