

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ventricular arrhythmias are a risk factor for sudden death among patients with post-infarction cardiomyopathy (CMP).1)2) Sudden arrhythmic death from ventricular tachycardia (VT) or fibrillation is thought to account for approximately one-third of deaths in post-infarction CMP patients.3)4) Sustained monomorphic VT is typically caused by reentry though a heterogeneous infarct scar, and will be the focus of this review. Primary5)6)7)8) and secondary9)10)11) prevention trials have shown that implantable cardioverter-defibrillators (ICDs) decrease mortality among this patient population. However, ICD therapies-particularly shocks-are associated with depression and anxiety,12) a decreased quality of life,12)13) increased healthcare utilization14) and mortality.15) In ICD clinical trials, the incidence of appropriate shocks for ventricular arrhythmias ranges from approximately 20% in primary prevention trials6)7) to 64% in the largest secondary prevention trial.9) In the ALTITUDE registry of 185778 ICD patients, the incidence of appropriate shocks was 8% in the first year and 23% in five years.16) Amiodarone, beta-blockers and sotalol have demonstrated modest efficacy in reducing shocks. However, in one randomized trial, the annual incidence of appropriate shocks in post-infarction CMP patients taking anti-arrhythmic medications remained at 6.7%.17)
Advances in catheter ablation and mapping technology have made catheter ablation an effective therapeutic option for patients with recurrent VT and appropriate ICD shocks. This article will discuss the pathophysiology of sustained monomorphic VT among patients with post-infarction CMP, and review the evidence and clinical practice of catheter ablation.
Pathophysiology of Post-Infarction Ventricular Tachycardia
Post-infarction VT is caused by reentry through diseased myocardium due to prior myocardial infarction. These areas of scar are comprised of fibrotic, unexcitable tissue, interspersed with areas of surviving, partially depolarizable myocytes (often referred to as "isthmuses" or "channels"), and areas of functional block that lead to slow conduction and unidirectional block critical to initiating reentry (Fig. 1). Scar sustaining post-infarction VT can be quite large, comprising up to 50% of the left ventricular (LV) surface area,18) can contain several isthmuses and exit sites, and can lead to multiple VTs from the same scar area. Surface electrocardiogram (ECG) QRS morphology of a given monomorphic VT reflects only its exit site, and mapping with intracardiac electrograms (EGM) or three-dimensional (3D) electroanatomic systems is required to identify the extent of the scar and its associated isthmuses or channels. Early physiologic studies found that most macro reentrant VTs have protected, narrow isthmuses that are required for maintenance;19)20) in 1990 Morady et al.21) first described the successful treatment of VT using radiofrequency (RF) catheter ablation in three patients.
Indications for Catheter Ablation
Patients with post-infarction CMP and ICDs who receive ICD shocks can be treated with either antiarrhythmic drugs or offered catheter ablation. In a patient without comorbidities who presents with ICD shocks for monomorphic VT, catheter ablation is a reasonable initial option at an experienced center, and may limit the long-term toxicities of antiarrhythmic drugs such as amiodarone. For patients already on antiarrhythmic drugs receiving ICD shocks, ablation is often the next best option. The European Heart Rhythm Association and Heart Rhythm Society have issued a joint expert consensus statement22) with specific indications for ablation (Table 1).
Current RF ablation catheters are irrigated with saline to cool the catheter tip-tissue interface and allow the delivery of adequate power without char formation.23) The first study of an irrigated catheter in patients with post-infarction VT demonstrated a 54% freedom from VT at mean 243-day follow-up.24) Other trials of irrigated catheters have shown freedom from recurrent VT in 51-53% of patients over 6-12-month follow-up.25)26) Catheter ablation has also been shown to be effective in patients with VT storm.27)
Previously, given the risk of undergoing an invasive procedure, catheter ablation of post-infarction VT was largely limited to patients with recurrent ICD shocks. However, two randomized clinical trials tested the strategy of prophylactic VT ablation at the time of ICD implantation. In the VTACH study,28) 107 patients with post-infarction CMP and stable VT were randomized to ICD versus ICD plus catheter ablation. At two years, 47% in the ablation group compared with 29% in the control group were free of VT. The SMASH-VT study29) also randomized patients who presented with VT (including unstable VT or VF) to ICD implantation with or without prophylactic VT ablation. Two-year freedom from VT was 88% in the ablation group compared with 66% in the control group. More importantly, the frequency of future ICD shocks was lower in the ablation group (9% vs. 31%; p=0.003). Neither study demonstrated a mortality benefit with prophylactic VT ablation, although there was a trend toward decreased mortality in the SMASH-VT study (9% vs. 17%; p=0.29). Therefore, in some patients without significant comorbidities who initially present with monomorphic VT, prophylactic VT ablation at an experienced center can be considered prior to ICD placement.
Pre-Procedural Considerations
Post-infarction VT catheter ablation procedures are often complex and may involve repeated induction and prolonged mapping of sustained VT. Careful procedural planning, taking into consideration anesthesia requirements, comorbidities, anticoagulation, and reference ECG data, can help to ensure success and minimize complications.
When possible, 12-lead ECGs of the "clinical VT" (defined as the VT morphology occurring spontaneously) should be obtained. VT morphology helps to localize the exit site of the re-entrant circuit from the protected isthmus, and helps with procedural planning. A right bundle branch block morphology in lead V1 identifies a LV exit site, whereas left bundle branch block morphology suggests a VT exit in the right ventricle or, more commonly, LV septum. More specific localization can be achieved using leads AVR and AVL to distinguish septal from lateral exit, leads II, III, and AVF to distinguish superior from inferior exit, and the precordial leads to identify an apical/mid/basal exit (Fig. 2). Surface ECG localization allows for procedural planning, particularly in terms of vascular access, and for guiding the initial mapping procedure. In patients for whom surface ECG tracings of VT are not available, ICD interrogation can be helpful to define VT cycle length and intracardiac EGM morphology. After inducing VT during the ablation procedure, real-time ICD EGM morphology may be compared to the stored ICD EGM to determine if induced VT is, indeed, the clinical VT.
Myocardial ischemia can increase the risks of VT ablation and potentially contribute to the slow conduction that sustains VT. It is, therefore, important to exclude myocardial ischemia with coronary angiography or a non-invasive stress test prior to any electrophysiology study. In the presence of ischemia, revascularization should be performed. Determining the location of any prior infarction using cardiac magnetic resonance imaging, nuclear imaging, or echocardiography is also helpful for guiding VT substrate mapping.
Antiarrhythmic medications should ideally be discontinued in advance of the procedure to maximize the chance of inducing VT. This may require hospital admission for with holding of antiarrhythmic medications in a safe environment. During mapping in the LV, anticoagulation is typically required to prevent thromboembolic phenomena, so consideration should be given to bleeding risks, particularly in patients on anti-platelet therapies. Post-procedurally, aspirin typically suffices, although a short course of warfarin may be considered when extensive LV ablation is performed and LV function is poor. Trans-thoracic echocardiography (preferably with contrast) should be performed to exclude mobile LV thrombus given the risk of embolization with catheter manipulation. However, the presence of laminated LV thrombus is not a formal contraindication.22) Patients who also have persistent atrial fibrillation (AF) should receive four consecutive weeks of therapeutic anticoagulation or transesophageal echocardiography prior to their procedure, as defibrillation during VT ablation may lead to cardioversion of AF, and the associated risk of thromboemboli. Transesophageal echocardiography may also be useful in elderly patients to exclude significant aortic atherosclerosis. The LV may be accessed either via the femoral artery in retrograde fashion through the aorta and aortic valve, or via the femoral vein transeptally and across the mitral valve. Transseptal access should be used in patients with significant peripheral vascular or aortic valve disease.
Post-infarction CMP patients with severely reduced systolic function may require hemodynamic support to safely undergo VT ablation. Options include intra-aortic balloon pump, Impella micro-axial blood pump (Abiomed, Inc., Danvers, MA, USA), peripherally-inserted Tandem Heart (CardiacAssist, Inc., Pittsburg, PA, USA), or cardio-pulmonary bypass. No formal guidelines or data predict the need for mechanical support, but it may be considered in patients with severely reduced systolic function {ejection fraction (EF) < 20%} in whom spontaneous VT is not hemodynamically tolerated. The drawbacks of hemodynamic support are added procedural complexities and additional risks with large-bore arterial access-of particular concern among patients with significant peripheral vascular disease. Ultimately in these patients, substrate modification techniques (described below), which do not require the need for mapping during sustained VT, may be preferable to using these devices.
Patients with implanted left ventricular assist devices (LVAD) experience an incidence of ventricular arrhythmias as high as 52% in one year.30) VT in LVAD patients may arise from the "suck-down" of the interventricular septum into the inflow cannula, a phenomenon more likely to occur in the setting of hypovolemia, and which must be excluded prior to the pharmacologic or catheter-based treatment of VT. Monomorphic VT in LVAD patients typically arises from pre-existing scar from the post-infarction CMP, or from reentry around the LV inflow cannula or its sutures. While sustained VT can be well-tolerated in patients with normally-functioning LVADs,31) catheter ablation may be beneficial in LVAD patients who suffer from symptoms or right heart failure in the setting of VT.32)33)
Mapping and Ablation of Ventricular Tachycardia
Sedation during VT procedures is often performed with the help of an anesthesiologist, and many centers prefer cardiac anesthesiology support for patients at high risk of hemodynamic deterioration. When possible, general anesthesia should be avoided as general anesthetics may suppress inducibility of VT.
Typically, the first step in VT ablation procedures is to attempt to induce VT with paced ventricular extrastimuli. In a minority of patients- 12% of subjects in the VTACH trial28)-VT is not inducible due to altered autonomic tone, antiarrhythmic medications, anesthesia or sedative medications. When VT is non-inducible, a limited "substrate modification" procedure may still be performed (as described below for "unmappable VT"). More commonly, even in patients who have one "clinical" VT morphology, multiple different VT morphologies can be induced. In the multicenter Thermocool trial,26) a median three different VTs were inducible per patient. These different VT morphologies may arise from different areas of scar, or may simply represent different exit sites from the same scar. VTs that are hemodynamically unstable are typically referred to as "unmappable" VTs, whereas VTs that can be induced and sustained without hemodynamic compromise are considered "mappable." This distinction largely dictates the approach to VT mapping, as activation and entrainment mapping require stable sustained VT.
Mappable ventricular tachycardia-activation and entrainment mapping
If sustained VT is induced, an activation map can be created by the manipulation of the mapping catheter to record the earliest area of activation. An electroanatomic mapping system is useful for tracking activation in a 3D space. A mapping catheter is moved point-to-point around the ventricle, comparing the timing of each point's QRS onset to the reference fiducial point on a surface ECG lead. The 3D map is color-coded to highlight the area of earliest activation.
Entrainment mapping is then performed near the site of earliest activation. Briefly, entrainment mapping involves intermittently pacing near areas of scar at a rate slightly faster than the VT rate. The response to pacing and pattern of resumption of VT after pacing help to identify the various components of the reentrant circuit (Fig. 3): entrance, isthmus, exit, inner loop, outer loop, adjacent bystander, or remote bystander.34)
After entrainment mapping, RF ablation is then typically performed focally at the critical isthmus site. This represents a narrow protected channel that is most likely to result in VT termination during ablation. These lesions may be extended to form a small 3-5 cm line to prevent VT recurrence. In some cases, ablation at an isthmus may "re-orient" the VT to take another path through the area of the scar to a different exit site with a slightly different morphology. Thus, entrainment mapping and isthmus ablation may need to be repeated over the same area of scar. It should be noted that after ablation of the mappable VT, many centers also perform additional substrate modification (discussed below).
Unmappable ventricular tachycardia-voltage and pace mapping
Approximately 70% of patients have hemodynamically unstable VT that precludes activation or entrainment mapping.26) For these patients, voltage and pace mapping are used during sinus rhythm to identify optimal sites of RF ablation.
Voltage mapping utilizes electroanatomic mapping to create a 3D map of the ventricle, color-coded to the voltage of the intracardiac EGMs recorded at each point. For bipolar voltage maps, prior studies have shown that the fifth percentile of normal voltages in healthy hearts is 1.5 mV. Voltages <0.5 mV have been shown to correlate with dense scar. Therefore, color-coding of electroanatomic maps is typically standardized to depict voltage ranges of >1.5 mV (healthy or "purple"), <0.5 mV (scar or "red"), and border zone (<1.5 mV and >0.5 mV) (Fig. 4). These bipolar ranges reliably depict the location of prior infarction. Voltage ranges can also be altered to identify potential "channels" of relatively higher voltage within scar that may represent a critical isthmus for sustaining VT.35)
When a 12-lead ECG of the clinical VT is available (either from patients' records or recorded after induction of a hemodynamically unstable VT at the start of the procedure), pace mapping can be performed by pacing from a catheter tip at various points near the suspected exit site of VT (often at the border zone of the scar identified by voltage map) until a pace map is identified that matches the morphology of the VT. RF ablation is then typically performed in a linear fashion through these matching pacemap regions in order to interrupt the presumed location of the VT circuit.
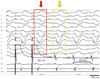
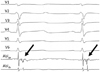
Intracardiac EGMs can also be scrutinized for low-amplitude, high-frequency signals that occur after the QRS complex, suggesting slow conduction (Fig. 5). Often called "late", "isolated", "delayed", or "diastolic" potentials, or "local abnormal ventricular activities", these potentials have been shown to correlate with infarct age,36) isthmus sites as identified by pace and entrainment mapping,37)38) and channels as identified by voltage mapping.35) Ablation of these potentials has been associated with a lower risk of recurrent VT in some series.39)40)
Ablation Strategies and Procedural Endpoints
Once optimal ablation sites are identified with the above mapping approach, irrigated RF energy is used to create lesions at powers ranging from 30-50 W. With externally irrigated catheters, attention should also be paid to patients' volume status, as saline infusion rates range 8-15 mL/min during ablation, and patients often receive over one liter of fluid.
It should be noted that there are no studies comparing the efficacy of the aforementioned approaches to mapping; most centers use a combination. Typically, after ablation of mapped sites, re-induction of VT is repeated with ventricular extrastimuli. Procedural endpoints used to define "successful ablation" include: 1) non-inducibility of the clinical VT, 2) non-inducibility of all VTs, and 3) elimination of all late potentials. In the Multicenter Thermocool trial, inducibility of any VT at the end of the procedure was associated with almost double the rate of VT recurrence, although there was no increased risk when the analysis was limited to inducible VTs that were faster than the clinical VT.26) Finally, an approach of empiric "scar homogenization" with endocardial and epicardial ablation of all abnormal potentials was shown to decrease VT recurrence when compared to standard endocardial mapping and ablation alone in one single center retrospective study,41) and this requires further investigation. Ultimately, the choice of the endpoint must be chosen based on procedural time and the patient's clinical status, as prolonged, repeated attempts at VT induction, pacing, and ablation may lead to adverse outcomes in the clinically brittle post-infarction CMP population. If stimulation is not performed at the end of a procedure due to hemodynamic instability, non-invasive programmed stimulation (NIPS) via the ICD can be performed one to two days later. Induction of clinic VT during NIPS correlates with a high likelihood of recurrent VT.42)
Epicardial ablation, while often necessary for non-ischemic CMP VT, is not routinely performed in post-infarction VT, since scar related to myocardial infarction is predominantly sub-endocardial. However, after unsuccessful endocardial ablation, epicardial mapping and ablation may be considered in post infarction CMP patients who have not undergone prior cardiac surgery (as prior surgery causes adhesions which increase the risk of subxyphoid epicardial access). Epicardial VT circuits are identified in approximately 10% of post-infarction VT studies, and are more often associated with prior inferior wall infarcts.43)
Complications
Multi-center studies of post-infarction VT ablation have demonstrated approximately 8% of major complication rates related to VT ablation, which is most often due to incessant VT.24)26) The most common complication is vascular injury (pseudoaneurysm, arteriovenous fistula, dissection), particularly with arterial access and retrograde aortic access of the left ventricle, occurring in approximately 2% of procedures.22)24)25)26)27) Stroke or transient ischemic attack occurs in 1-2%, highlighting the need for judicious anticoagulation with LV mapping and ablation. Cardiac perforation and tamponade can occur in 1%.24)25)26)27) In patients with septal VTs, ablation near the His bundle can lead to heart block.24) Heart failure exacerbations may occur after post-infarction VT ablation,26) and may be due to irrigation volume infused or "stunning" effects from numerous RF lesions. The SMASH-VT trial, however, routinely monitored LV EF before and after VT ablation, and found no difference between pre-ablation EF and EF at three and 12 months post-ablation.29) Peri-procedural mortality ranges from 0 to 3% in major clinical trials,24)26)28)29) and was 1.75% in a recent registry-based study.44)
Emerging Technologies
Remote magnetic navigation ("Stereotaxis") techniques have gradually expanded to electrophysiology procedures, and have demonstrated some efficacy in post-infarction VT.45) Remote navigation offers the hope of reducing fluoroscopy and procedure times. While remote navigation can acquire detailed LV substrate maps, modest contact force with the LV endocardium may limit the depth of delivered ablation lesions.
Scar in the inter-ventricular septum often presents a challenge for endocardial ablation, as the protected VT circuit can be located deep in the septum, and may not be approachable from the right or LV endocardium or epicardium. In this setting, a cooperative effort between electrophysiologists and interventional cardiologists may be required to ablate the VT with transcoronary ethanol infusion.46) Other approaches for deep septal VTs include bipolar ablation on both sides of the septum,47) or use of a saline-infused RF needle ablation catheter.48)
Summary
Post-infarction VT represents a significant source of mortality and symptoms, particularly among patients with ICDs; antiarrhythmic medications such as amiodarone provide modest efficacy with significant side-effects and toxicities. RF catheter ablation of post-infarction VT results in approximately 50-75% freedom of VT after one year, as well as a significant reduction in the frequency of ICD shocks. A variety of mapping and ablation approaches may be used depending on inducibility and hemodynamic tolerance of VT, targeting either critical isthmuses of macro-reentrant loop, or late potentials. Procedural risks can be reduced by careful planning and patient selection.




 XML Download
XML Download