

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Most coronary artery origin abnormalities are incidentally determined during coronary angiography. In the adult population, its prevalence is reported to be approximately 0.3 to 1.3% in the largest registry.1) These abnormalities are usually asymptomatic and have no clinical significance. However, some cases of coronary artery abnormalities are related to severe life-threatening events such as myocardial ischemia, arrhythmia and acute myocardial infarction.2) We report an uncommon case of an anomalous origin of the left coronary artery (LCA), a single coronary artery, arising from the right sinus, with angina pectoris and palpitations.
Case
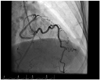
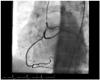
A 48-year-old woman presented with exertional angina and palpitations for a long time. She a had medical history of hypertension and dyslipidemia, and a family history of coronary artery disease. Her father had a heart attack at an early age. The electrocardiogram showed normal sinus rhythm and nonspecific ST-T wave changes. Labaratory examinations were unremarkable. The exercise electrocardiogram showed dynamic changes with ST-segment depression in the V 1-4 leads. Echocardiography revealed preserved left ventricle systolic function and concentric left ventricle hypertrophy. The coronary angiography procedure was started with a LCA cannulation attempt, but left anterior descending coronary artery and Cx imaging was unsuccessful even though contrast was injected into the left coronary sinus. The right coronary artery was cannulated and visualized with a right Judkins catheter. At this time, we noticed the left coronary arteries arising from the right sinus of Valsalva. The right Judkins catheter was gently pull back and the left coronary arteries were clearly visualized (Figs. 1 and 2). There was no significant stenosis of any of the three coronary trees. Coronary CT angiography confirmed that the left coronary arteries arose from the right sinus of Valsalva and that all three coronary arteries originated from the single sinus (Fig. 3). The patient was managed with conservative treatment and has had no symptoms on clinical follow-up.
Discussion
Coronary anomalies affect less than 1% of the general population. Anomalous origin of LCA from the right sinus of Valsalva is the rarest anomaly, with a reported prevalence of 0.02-0.03% according to studies. The isolated origin of a single coronary artery is very rare, with an incidence of 0.04% to 0.23%.3) Most of these coronary artery anomalies are generally asymptomatic; however, some can cause severe potentially life threatening events. Understanding anatomic coronary variations is important in determining anomalous origins that are related to sudden cardiac death.4)
Single coronary artery has been defined angiographically by Lipton et al.5) according to the origin from the coronary artery. The modified Lipton classification includes features such as the anatomical distribution, the ostial location, and the course of the transverse trunk.
Anomalous origin of the LCA from the right sinus of Valsalva is associated with sudden death in some cases (59%) because an anomalous artery between two great vessels is related with acute myocardial infarction and sudden cardiac death.6) The acute angle of the ostium increases the risk of sudden cardiac death. The anomaly determined in our patient seemed to be potentially malignant, but without marked compression between the great arteries.
The management of patients with an anomalous origin of coronary artery includes observation, medical treatment, coronary stent implantation and surgery repairment. However, in our case medical treatment was chosen due to the absence of compression of the coronary arteries by the great arteries, and the lack of acute ostial angulation. The patient was treated with a beta blocker and nitroglycerin because of the angina pectoris and palpitations, and she has remained asymptomatic for 1 year on follow-up.
Although cardiac catheterization is generally accepted as the gold standard for the evaluation of coronary anomalies, CT angiography has recently emerged as an effective and noninvasive method for performing imaging of the origin of the coronary arteries.
In conclusion, the determination of the anomalous origin of the coronary artery and the cardiovascular system is of great clinical importance due to its severe life-threatening complications. The new imaging modalities that have emerged enable the accurate visualization of the anatomical configurations and the detection of structural malformations. Most of the structural cardiovascular abnormalities are incidentally detected and are asymptomatic; however, a few are potentially significant and can trigger sudden death.

 XML Download
XML Download