

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Heart failure (HF) is responsible for an increasingly large proportion of cardiovascular morbidity and mortality. Hypertension and coronary heart disease (CHD) are considered to be the main causes of HF.1) Diabetes, smoking, obesity, and dyslipidemia are also associated with HF.2-5) The main features of metabolic syndrome (MetS) include insulin resistance, hypertension (high blood pressure), cholesterol abnormalities, and increased risk of clotting. Patients are likely to be overweight or obese. MetS, which comprises a cluster of cardiovascular risk factors, also increases the risk of cardiovascular disease (CVD) and many of its components can lead to HF. Sometimes medications for HF can affect the components of MetS. Likewise, the treatment of MetS can also affect the prognosis of HF.6)
The association between MetS and HF has been less studied than that between MetS and CHD. It is unknown whether MetS is associated with HF independent of myocardial infarction (MI) and diabetes mellitus. Therefore, the aim of the present study was to investigate the prevalence of MetS in patients with HF and determine whether the presence or absence of MetS is associated with the clinical outcome of HF.
Subjects and Methods
Study population and grouping
From the nationwide prospective Korea HF Registry (KorHFR), 3200 HF patients were enrolled from 24 centers in Korea between Jan. 2005 and Oct. 2009. The patients had been admitted to hospital for HF that was confirmed at the time of discharge. The data was recorded via a web-based electronic capture system, which also recorded follow up events. Data collection and audition were performed by the KorHF Registry Steering of the Korean Society of Heart Failure.
The patients were divided into two groups according to the presence or absence of MetS at the time of admission, with MetS defined as the presence of three or more criteria from the National Cholesterol Education Program (NCEP) and the American Association of Clinical Endocrinologists criteria (AACE). Patients were separated into group I (presence, n=1141) and group II (absence, n=2059).
The study protocol was approved by the Institutional Review Board or ethics committee at each participating hospital. Approval was obtained from Chonnam National University Hospital (No=06-타).
Definitions of the metabolic syndrome and other risk factors
The present study was based on the NCEP, AACE, and American Heart Association (AHA) definitions of MetS, which all include subjects with diabetes mellitus in their definitions.7)8) With respect to obesity, body mass index (BMI) was used according to the AACE criteria. MetS was defined as presence of ≥3 of the following criteria: high blood pressure (≥130 mm Hg systolic or ≥85 mm Hg diastolic blood pressure) or taking blood pressure medication, impaired glucose tolerance (fasting blood glucose ≥110 mg/dL) or diagnosed diabetes, obesity (BMI >25), triglycerides >150 mg/dL, high density lipoprotein-cholesterol (HDL-C) <40 mg/dL in men or <50 mg/dL in women. Weight, height, and blood pressure were measured at baseline. BMI was calculated as the weight in kilograms divided by the square of the height in meters. Smoking status was defined as current smoking. With respect to alcohol consumption, subjects were classified as alcohol users or non-users.
Laboratory tests
Blood samples to assess the serum lipid profile and glucose were obtained in the morning after a 12-hour overnight fast. High sensitivity C-reactive protein (hs-CRP) was measured by the immunoturbidimetric CRP-Latex (II) high-sensitivity assay using an Olympus 5431 autoanalyzer (Olympus America Inc., Melville, NY, USA). Electrocardiography was performed at first visit day. Serum N-terminal-pro-brain-natriuretic peptide (NT-pro-BNP) was measured using an electrochemiluminescence sandwich immunoassay method with an Elecsys 2010 analyzer (Roche Diagnostics, Mannheim, Germany). The analytic range of the NT-pro-BNP assay extends from 5 to 35000 pg/mL.
Echocardiography
A comprehensive two-dimensional, spectral and color flow Doppler echocardiographic examination was performed at admission. Indices of global and segmental systolic function and diastolic function were obtained. Left ventricular (LV) size and ejection fraction (EF) were determined using the Teicholz method or modified biplane Simpson's method by orthogonal apical views (2 and 4-chambers).9)10)
Pulse wave Doppler curves of blood flow and tissue Doppler were assessed by the apical 4-chamber view. Mitral diastolic inflow velocities were obtained at the tip of leaflets; LV outflow systolic flow curves were obtained just below the aortic valve closure plane. The ratio of mitral E/A wave diastolic velocities, deceleration time of early LV diastolic filling and E/E were also checked. Valvular stenosis or regurgitation was evaluated by color Doppler imaging.
Statistical analysis
The Statistical Package for the Social Sciences for Windows, version 15.0 (Chicago, IL, USA) was used for all analyses. All values were expressed as a mean±standard deviation. Comparisons of means between the groups were done by using a Student t-test and analysis of variance as appropriate. A p<0.05 was considered statistically significant. Kaplan-Meier probability was tested by using the log-rank method.
Results
Clinical characteristics
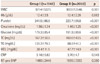
A total of 3200 HF patients (68.2±15.5 years, male=50%) were enrolled in the KorHFR between Jan. 2005 and Oct. 2009. The observational period was mean 90.5 days (range=0 to 1180 days). The prevalence of MetS was 35.7% in patients with HF and was higher in females (56.0%). Weight, BMI, systolic and diastolic blood pressure were higher in group I (presence of MetS) than in group II (absence of MetS). There were no significant differences in age, heart rate, and New York Heart Association (NYHA) classification between the two groups. Comorbidities such as hypertension, diabetes, and chronic kidney disease were more frequent in group I than in group II. Prior HF, valvular heart disease, and post valve surgery status were more frequent in group II. Prior coronary intervention or bypass surgery, arrhythmia, and chronic lung disease were not affected by the presence of MetS (Table 1).
Etiology of heart failure
Ischemic HF was significantly more frequent in group I than in group II. Valvular or idiopathic causes were less frequent in group I than in group II (Fig. 1A). MetS was present in 40.4% of the patients with ischemic HF compared to 27.5% of patients with valvular heart disease.
Laboratory findings
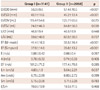
The laboratory findings of the patients at admission are summarized in Table 2. The levels of white blood cells, platelets, creatinine, glucose, and cholesterol were higher in group I than in group II. The levels of NT-proBNP and hs-CRP were similar between the two groups.
Echocardiographic findings
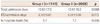
In echocardiographic findings, LV dimension and volume were smaller in group I than in group II. EF was higher in group I than in group II. Diastolic parameters were not different between the two groups except for mitral annular velocity (Table 3).
The prevalence of systolic HF was significantly higher in group II, whereas diastolic HF with preserved EF above 50% was higher in group I (Fig. 1B).
Short and mid-term events
During the admission period, half of the patients with HF were supported in an intensive care unit (ICU). Total admission duration and the rate of ICU care were similar across the two groups. All causes of death occurred in 197 cases (6.2%) during the follow up period. Mortality was lower in group I than in group II (Table 4).
The incidence of cardiac arrest, in-hospital infection, cerebrovascular accident, bleeding complication, and new onset malignant arrhythmia during admission were not different between the two groups. During the follow-up period, the cumulative survival rate was significant higher in group I than in group II (log rank p=0.010). However, there was no difference in the re-admission rate between the two groups at one and three-month follow up (Fig. 2).
Discussion
Heart failure is a syndrome rather than a diagnosis of one single pathology. Many HF patients succumb to progressive pump failure and fluid congestion.11) Results from prospective cohort studies have indicated that older age, male sex, hypertension, diabetes, obesity, valvular heart disease, and CHD are important risk factors for CHF.12)13) These factors must be carefully monitored and controlled because they put extra strain on the heart and can lead to HF. These cardiovascular risk factors were also associated with MetS. The relationship between MetS and HF has been relatively rarely reported. Nevertheless, many components of MetS can lead to HF, and are associated with insulin resistance, inflammation, and fluid accumulation. Furthermore, medical treatment of HF can affect insulin sensitivity and treatment of the components of the MetS may affect HF.
Metabolic syndrome, which comprises a cluster of cardiovascular risk factors, increases the risk of CVD. MetS involves complex conditions, including obesity, high blood pressure, and low levels of HDL-C. A person with MetS is at an increased risk of developing CHD, stroke, and diabetes.14)
There are several criteria of MetS based on the WHO,15) the NCEP,16) the International Diabetes Federation,17) and the AHA and the AACE, all of which include subjects with diabetes in their definitions.
With respect to obesity, we used BMI rather than waist circumference because of lack of information on waist circumference. Body weight tends to be increased at initial admission compared with that in usual condition due to fluid accumulation. We analyzed the data according to the measured body weight, which could affect how we examined the incidence of MetS.
However, BMI had a somewhat higher hazard ratio in predicting HF than did waist circumference in the present study. A recent Swedish prospective study in 1187 male subject aged over 50 years found that BMI had almost same heart rate as waist circumference for incident congestive HF.18) Therefore, BMI was deemed to be acceptable for definition of MetS according to the AACE criteria. The definition of overweight tends to be given as BMI ≥25 kg/m2 in the Korean population.19)20)
In a recent study concerning patients with HF, obesity appeared to be associated with a better overall clinical prognosis and patients with more severe HF tended to have lower BMI compared with age and gender-matched control subjects21) and higher BMI was associated with a better survival rate in patients with stage IV HF.22) Our study also showed that the percentage of advanced stage HF (NYHA≥III) was significantly higher in group I.
Heart failure risk increases with advancing age.23-25) HF is the most common reason for hospitalization in people age 65 years and older. The mean age of the patients in this study was 67 years. However, there was no significant difference according to the presence of MetS in our data. It is known that men are at higher risk of HF than women.26) However, our data showed female predominance in the MetS group. Women are more likely to develop diastolic HF than their male counterparts, which is often a precursor to systolic HF. Subjects with MetS have been reported to have higher LV mass and more concentric LV hypertrophy, as indicated by higher relative wall thickness.27)
This morphologic change is often thought to characterize patients with HF in the setting of a preserved EF. In our data, HF with preserved systolic function was more frequent in the MetS group. In the laboratory findings, the levels of white blood cells, platelets, creatinine, CRP, and lipid were higher in the MetS group. This might be due to the role of inflammation. In a previous study, all subjects with MetS were associated with a 1.45-1.74-fold risk for incident HF after adjustment for confounding factors. When subjects with interim MI during the follow up and those with prevalent diabetes were excluded, MetS was significantly associated with a 1.37-1.87-fold risk for incident HF after adjustment for confounding factors.28)29)
Despite the increased cardiovascular risk it involves, MetS was not associated with mortality and morbidity in patients with HF in our study. Total admission duration, the duration of ICU care, rate of re-admission and the mid-term mortality were not significantly different according to the presence of MetS. In addition, in-hospital mortality was lower in the MetS group. The question is whether MetS plays a protective role in HF prognosis. It is important here to note that HF patients with MetS may be detected earlier due to multiple risk factors at a less severe level of HF and this may affect the prognosis. This study showed that MetS could affect HF via a different route than is the case in the usual mechanism. This may involve micro vascular ischemia leading to maladaptive subclinical cardiac structural changes.
A limitation of our study is that we carried out retrospective analysis of the data present in the registry. Therefore we could not conduct intervention or modulation of risk factors. We did not know the precise details of any substantial reduction of weight, or control of blood pressure, glucose, and lipid levels, which change the cardiac structure and function as well as the clinical manifestations of HF. Because the Echocardiography Core Lab was not used during the registry process, the echocardiographic data may not be standardized. Further studies are needed to elucidate the mechanism that underlies the relationship between MetS and HF prognosis.



 XML Download
XML Download