

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Arterial stiffness is a recognized factor associated with an increased risk of coronary artery disease (CAD) and is currently used as a predictive factor, especially as an index predictive of target organ damage in hypertension.1-3) According to the Framingham Heart Study, systolic blood pressure (SBP) is positively associated with coronary heart disease, whereas diastolic blood pressure (DBP) has a negative relationship. As a result, pulse pressure widening was found to be the most significant risk factor of coronary disease and mortality.4) It is already recognized that arterial stiffness, the main mechanism underlying pulse pressure widening, is an independent risk factor for cardiovascular disease and stroke.5)6)
Numerous methods have been developed to assess arterial stiffness, including pulse wave velocity (PWV) and augmentation index (AI). PWV is a widely used, non-invasive method for evaluating arterial stiffness and atherosclerosis. Increased PWV is a marker of atherosclerosis and has been shown to reliably predict the presence and extent of atherosclerotic vascular disease.7)8)
The AI reflects arterial stiffness by pulse wave analysis and is a hemodynamic index representing arterial stiffness. AI is known to increase at the early phase of atherosclerosis, making it a candidate screening tool for assessing the risk of cardiovascular disease. Numerous studies have focused on this potential. Although some studies have suggested that the AI is associated with cardiovascular risk factors that correlate with cardiovascular disease, others have demonstrated no such relationship. According to Hope et al.,9) the AI is not associated with the extent of coronary disease, nor its severity. Therefore, the association between AI and cardiovascular disease has not been firmly established and remains a topic of great debate.4)9-11) Despite several studies on the relationship between PWV or AI and the prevalence of coronary heart disease, relatively few studies have simultaneously compared the correlation between these coronary artery indices and the status of coronary arteries as assessed by coronary angiography. Therefore, this study concurrently investigated the association between PWV and peripheral augmentation index (pAI) and CAD.
Subjects and Methods
We analyzed medical records from our coronary laboratory for data on CAD, and from our non-invasive laboratory for data on PWV and pAI. Patients who visited Wonju Severance Christian Hospital from May 2010 to March 2012 were enrolled. A total of 7020 and 6373 patients underwent coronary angiography and PWV measurement, respectively. Among them, 1030 patients underwent both tests, and after excluding patients with missing data, the final analysis included 965 patients (Fig. 1).
Diagnosis of coronary heart disease
Coronary heart disease was diagnosed when an occlusion of greater than 50% of the lumen of any major coronary artery was found on coronary angiography. The patients were classified based on the extent of disease as: none/minimal or 1-, 2-, or 3-vessel disease, depending on the number of vessels involved.
Clinical data
The patients' age, sex, height, weight, pulse rate, diastolic and SBP, and medical history (hypertension, diabetes mellitus, chronic renal failure, hypertension, myocardial infarction, and smoking status) were obtained from the coronary angiography database of Wonju Severance Christian Hospital. Hypertension was defined as SBP ≥140 mm Hg, DBP ≥90 mm Hg, or current use of antihypertensive medication.
Pulse wave velocity and augmentation index
Pulse wave velocity was measured using a VP-1000 (Colin Co. Ltd, Komaki, Japan), and AI was measured using a HEM-900AI (Omron Healthcare Co. Ltd, Bannockburn, IL, US). PWV, blood pressure, electrocardiogram, and heart rate were simultaneously measured and recorded automatically. Electrodes were attached to the left sternum and the cuffs were closed on each patient's arm and ankle. Volume pulse form was derived from a plethymographic sensor connected to the cuff, and blood pressure was measured using an oscillometric pressure sensor. PWV was defined as the ratio of the distance between two points and the pulse transit time. The AI was derived from the pulse wave analysis measured from the brachial artery to the ankle. All values were measured during regular sinus rhythm within seven days after coronary angiography. Patients with peripheral artery disease (ankle brachial index <0.9) were excluded.
Statistical analysis
Data are presented as mean±standard deviation unless otherwise specified, and frequency was calculated as a percentage. Prior to analysis, the patients were divided into two groups: with and without CAD. We assessed the risk of CAD with respect to brachial-ankle pulse wave velocity (baPWV) and pAI and analyzed differences in the severity of coronary disease (none/minimal or 1-, 2-, or 3-vessel disease). Quantitative analysis of the clinical indices and complications was performed with Fisher's exact test, and the odds ratio (OR) of CAD is presented with the 95% confidence interval (CI). The risk of CAD in the two groups was calculated by multivariate logistic regression analysis. All statistical analyses were performed with Statistical Package for the Social Sciences version 18.0 (SPSS Inc., Chicago, IL, USA), and p less than 0.05 were considered statistically significant.
Results
Clinical characteristics of subject groups
Out of a total of 965 patients, 468 (48.5%) were diagnosed with coronary heart disease (Table 1). The study included 562 males and 403 females with a mean age of 63.7±11.6 years. The mean height and weight were 166.8±10.0 cm and 63.9±11.3 kg, respectively, and 608 patients (63.0%) were hypertensive. The number of patients with a history of smoking, diabetes, and hyperlipidemia was 388 (40.2%), 239 (24.8%), and 288 (29.8%), respectively.
The mean systolic and DBP was 126.8±17.4 mm Hg and 73.2±12.0 mm Hg, respectively. The mean pAI, adjusted for 75 pulses (pAI75), was 74.8±15.8% and the median baPWV was 16.2±3.5 m/sec.
Pulse wave velocity, peripheral augmentation index, and clinical features according to presence or absence of coronary artery disease
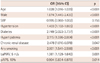
Patients with CAD had a mean age of 65.6±10.4 years, significantly higher than those without CAD. In addition, the proportion of males was higher in the CAD group (66% vs. 50.9%, p<0.05). The mean DBP was significantly lower in patients with CAD (71.1±12.2 mm Hg vs. 75.1±11.5 mm Hg, p<0.05), and the SBP was also lower (125.9±18.1 mm Hg vs. 127.6±16.6 mm Hg). The CAD group had a significantly higher proportion of patients with a history of hypertension (67.3% vs. 59%, p<0.001) and diabetes (34.2% vs. 15.9%, p<0.001). Furthermore, patients with CAD tended to have an increased history of myocardial infarction, cerebrovascular disease, coronary angioplasty, and smoking (Table 1).
The mean baPWV value for the CAD group was 16.6±3.5 m/sec, which was significantly higher than that in the control group (15.9±3.4 m/sec). However, the mean pAI75 for the CAD group was significantly lower than that of the control group (73.5±15.9% vs. 76.0±15.7%).
Pulse wave velocity and augmentation index according to severity of coronary artery disease
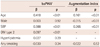
Peripheral augmentation index and baPWV were compared according to the severity of CAD (none/minimal or 1-, 2-, or 3-vessel disease) (Table 2). baPWV showed a significant positive correlation with the severity of CAD (none/minimal: 15.9±3.4 m/sec; 1-vessel disease: 16.2±3.3 m/sec; 2-vessel disease: 16.8±3.4 m/sec; 3-vessel disease: 17.3±4.0 m/sec, p<0.001). However, neither pAI75 (p=0.063) nor average pAI (p=0.131) was significantly correlated with the severity of CAD.
Correlation of pulse wave velocity and augmentation index with traditional risk factors
The correlation between baPWV or pAI and traditional risk factors was analyzed by linear regression. Age, SBP, and type 2 diabetes mellitus were significantly associated with baPWV; however, hyperlipidemia, smoking status, and sex were not significant factors in the multiple linear regression analysis. Age, female sex, and SBP showed a significant positive correlation with pAI (Table 3). Old age was the strongest independent risk factor for high baPWV (OR: 4.871, CI: 3.428-6.922, p<0.001). Hypertension (OR: 1.912, CI: 1.387-2.636, p<0.001) and diabetes (OR: 1.873, CI: 1.349-2.601, p<0.001) were also significantly correlated with baPWV (Table 4).
Logistic regression analysis of risk factors for coronary artery disease
A logistic regression analysis was performed using the variables found to be significantly different in patients with CAD (Table 1), specifically: age, sex, SBP, history of hypertension, history of diabetes, history of dyslipidemia, history of smoking, pAI75, and PWV (Table 5).
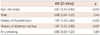
By univariate analysis, the traditional risk factors of coronary heart disease all demonstrated a significantly high OR {age (OR: 1.028, CI: 1.016-1.039, p<0.001), male sex (OR: 1.874, CI: 1.445-2.430, p<0.001), hypertension (OR: 1.433, CI: 1.102-1.865, p<0.001), diabetes (OR: 2.749, CI: 2.022-3.737, p<0.001), dyslipidemia (OR: 2.115, CI: 1.596-2.598, p<0.001), chronic renal disease (OR: 2.478, CI: 1.010-6.078, p=0.047), and history of smoking (OR: 1.395, CI: 1.057-1.840, p<0.001)}. pAI75 was associated with a reduced OR for CAD (OR: 0.904, CI: 0.834-0.979, p=0.014), whereas PWV demonstrated a significantly positive OR (OR 1.361, CI: 1.129-1.640, p<0.001).
Discussion
Recently, numerous researchers have taken an interest in arterial stiffness, and a number of related studies have been performed. These studies have found that increased arterial stiffness is a useful predictive factor that is associated with clinical events, not only in a hypertensive patient group but also in populations with type 2 diabetes or end-stage renal disease, and in the geriatric and general population.7)12-15) Our study is unique in that it simultaneously compared PWV and peripheral augmentation with different manifestations of CAD in a large population.
Pulse wave velocity is a well-known independent predictive factor of cardiovascular disease;1) however, few studies have investigated the difference in PWV according to the extent of coronary vessel disease. We found that baPWV increased according to the severity of CAD (none/minimal, 1-vessel, 2-vessel, or 3-vessel disease) (Table 2). This suggests that baPWV not only contributes to the presence of CAD, but also to the progression of cardiovascular disease. A similar result was observed in a study performed by Mattace-Raso et al.,1) although the sample size of their study was small (40 patients). Our study included 965 patients and our data may therefore be more meaningful.
In univariate analysis, baPWV was found to be a potentially useful independent predictive factor, similar to age, male sex, hypertension, diabetes, dysplipidemia, and smoking (Table 5).
On the other hand, pAI was significantly lower in patients with CAD (Table 1). This is contrary to the results of previous studies, which demonstrated elevated AI in early atherosclerosis and suggested an association between the pAI and CAD. There are several possible explanations for the decreased pAI in our patients with CAD.
First, the antihypertensive drug used in these patients could be a confounding factor. In our study, patients with CAD were found to have lower SBP than those without CAD because of the greater use of antihypertensive medication. Because pAI is positively correlated with SBP,16) this finding suggests that antihypertensive treatment could affect the pAI by lowering the blood pressure.
Second, as mentioned above, the patients in this study were older than the general population. Mattace-Raso et al.1) reported that the pAI increases with age until about 55 years, and slowly decreases down to a plateau thereafter. In our study, the mean age of the enrolled patients was 63.7±11.6 years. It is known that cardiovascular risk is greater among elderly men, and the decrease in pAI in our patients with CAD may be explained by this finding.
Third, pAI was significantly greater in females than in males. pAI tends to be overestimated among females because of their shorter height, arms, and legs. Since male sex is a major risk factor of CAD, the ratio of females was higher in the non-CAD group (49.4% vs. 34.0%), and this may have led to a higher average pAI value.
Lastly, pAI is a parameter derived from the reflected wave through pulse wave analysis, rather than a directly measured value. Therefore, the results might be influenced by the equipment, the measurement, and the patient. Furthermore, the current measurement method has not been validated, which may have resulted in measurement bias.
This study has several limitations. First, baPWV reflects arterial stiffness, which is influenced by various factors, including age, gender, and hypertension.17) In addition to applying large mechanical stress to the vascular wall as a result of high intravascular pressure, hypertension leads to growth of vascular smooth muscle that is associated with elevated levels of catecholamine, angiotensin II, and other cytokines, causing proliferation of fibrous protein within the tunica intima and loss of elasticity, both of which contribute to an increase in arterial stiffness.17)18) Because both age and hypertension contribute more strongly to coronary heart disease than baPWV, the influence of baPWV on CAD may have been reduced after adjusting for these factors.
Second, the study group consisted of high-risk patients. This study was performed on symptomatic patients who underwent coronary angiography, not on the general population. The median PWV for this group was 16.2±3.5 m/sec, which is higher than that reported by Han et al.8) in a study performed in a Korean population (11.23±5.10 m/sec), and the subjects' mean age was also higher (63.7±11.6 years).
In conclusion, increased baPWV and decreased pAI were associated with the presence of CAD in the elderly. pAI may be decreased in elderly and male patients with cardiovascular disease and may be attributable to the aforementioned confounding factors, such as age and history of anti-hypertensive medications, rather than an actual decrease in arterial stiffness. Therefore, considerations of these confounding factors must always be made when utilizing pAI in clinical practice. In addition, this study targeted high-risk patients, and a large-scale epidemiologic study involving the general population is necessary.



 XML Download
XML Download