

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Since its first description in 1838,1) cardiac diverticulum has been rarely reported, particularly when first diagnosed in adulthood.2)3) Although classic clinical features include congenital malformations involving the abdominal wall, sternum, diaphragm, pericardium, limb and myocardium, isolated left ventricular (LV) diverticulum is also described in about 30% of the cases. The differentiation of isolated apical diverticulum from apical aneurysm is a great challenge, particularly when it is first found in adulthood. We describe here an adult case of isolated left apical diverticulum that could not have been accurately diagnosed in the absence of cardiac magnetic resonance (CMR) technique.
Case
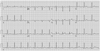
A 30-year-old woman was referred to our center with complaints of headache and right side weakness. Her medical history was unremarkable except for intermittent migraine attacks. She had no clinical risk factors for cerebrovascular disease. Small multifocal cerebral infarctions were found in her brain through brain magnetic resonance imaging. With suspicion of a cardiac source of embolism, transthoracic echocardiography was performed, which revealed apical akinetic movement with a band-like structure (arrow in Fig. 1A) in the LV. LV opacification with echocardiographic contrast showed no evidence of apical thrombi (Fig. 1B).4) Initial electrocardiogram did not suggest any sign of apical aneurysm, like ST elevation in anterior leads (Fig. 2). Computed tomographic thoracoabdominal angiography revealed normal findings, including no atherosclerosis (Fig. 3). In addition, she was young and had no risk factors for coronary artery disease, suggesting the impression that the chance for myocardial infarction was not high. For further evaluation of LV apex, CMR was ordered. The CMR identified a broad-based apical diverticulum (2.6×3.0 cm-sized) with mechanical activity, nearly synchronous with LV activity (Fig. 4A and B), along with an LV ejection fraction of 43%. Interestingly, delayed enhancement of CMR (DECMR) conveyed high signal intensity in some parts of diverticulum (Fig. 4C, D and E). She was finally diagnosed with a huge, isolated LV apical diverticulum with mixed muscular and fibrous type. On anticoagulation with warfarin, she was given permission to leave the hospital.
Discussion
Echocardiography is believed to be the first-line imaging modality for cardiac evaluation and can offer numerous invaluable information of the heart, including anatomy, function and hemodynamics. However, a thorough evaluation of LV apex with echocardiography is sometimes challenging due to its close proximity to the position of the echocardiographic probe. Moreover, an accurate tissue characterization with echocardiography cannot be successful. CMR can overcome this limitation and, almost always, provide clear LV apical images. In addition, DE-CMR offers histologic information on the myocardial tissue of interest, especially the presence or absence of fibrous tissue.5)6) With these 2 unique abilities, CMR is able to establish the diagnosis of LV diverticulum and its types (i.e., fibrous or muscular). It can differentiate diverticulum from aneurysm as well. In the present case, without CMR, LV apical diverticulum would have been misdiagnosed with apical aneurysm. However, thanks to the unique CMR ability of tissue characterization, the fact that a mixture of fibrous and contractile myocardial tissues constitutes apical diverticulum, which could not be achieved even using contrast echocardiography, could be identified. Therefore, we believe that CMR should be regarded as a "terminator" of cardiac imaging modalities in the evaluation of LV apex and, as such, be used more actively in our daily clinical practice in order to establish a proper diagnosis of LV apical pathology.



 XML Download
XML Download