

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Since 1990, a number of studies have reported that the inflammatory process is an important contributor to atherosclerosis and the vulnerability of atherosclerotic plaque. Among many inflammatory markers, high-sensitivity C-reactive protein (hs-CRP) is the most extensively studied biomarker of inflammation in cardiovascular disease.1) The results from many studies have shown a significant association between the elevated plasma level of hs-CRP and the severity of atherosclerosis, the incidence of cardiovascular events in individuals with risk factors, and the risk of recurrent cardiovascular events among patients with established coronary heart disease.2)3)
The role of hs-CRP as a predictor of the prognosis of cardiovascular disease has also been studied by many investigators. Many studies have found a strong positive correlation between the baseline level of hs-CRP and the incidence of future acute coronary events among stable angina pectoris patients.4-7) The Prevention of Events with Angiotensin-Converting Enzyme inhibitor trial divided 3771 stable angina pectoris patients according to the level of hs-CRP and evaluated the outcomes of cardiovascular death, myocardial infarction (MI), or stroke over a mean follow-up period of 4.8 years. The results showed that a higher level of hs-CRP was closely associated with a higher rate of cardiovascular events.8)
Contrary to the definite predictive value of hs-CRP in stable angina pectoris patients, there remains controversy about the predictive role of hs-CRP after acute MI. A study evaluated 448 acute MI patients and showed that the baseline level of hs-CRP measured 12-24 hours after the onset of symptoms had a significant association with 30-day mortality, larger infarct size, and more frequent heart failure.9) However, there were conflicting results observed between the two studies. A study enrolled 483 patients and revealed no definitive association between the level of hs-CRP measured within 6 hours from symptom onset and death and non-fatal MI in the following 30 days.10) The other study reported that an elevated level of hs-CRP measured within 6 hours from symptom onset had no significant impact on mortality at three years.11)
The main difference between these studies was the interval from the onset of symptoms to the measurement of hs-CRP. Therefore, we hypothesized that the different time interval was the cause of these different results and evaluated the impact of ischemic time on the predictive value of hs-CRP in ST-segment elevation myocardial infarction (STEMI) patients to investigate the reason for these conflicting results.
Subjects and Methods
Study population
Our study enrolled 5123 STEMI patients treated by primary percutaneous coronary intervention (PCI) from August 2008 to July 2011, consecutively. All enrolled patients were transported immediately to hospital for coronary angioplasty, where indicated. Angioplasty was performed according to the local standard protocol with the intention of restoring blood flow in the infarct-related artery as soon as possible. The data was derived from Korean Working Group in Myocardial Infarction (KORMI), which is a multi-centered and ongoing observational study designed to collect demographic, clinical, treatment, and outcome data on patients with acute MI. Because the KORMI is an anonymous observational study, no informed consent is required from participating patients by the institutional boards at any of the participating institutions.
This study included patients with a diagnosis of STEMI: a rise and fall of serum cardiac biomarkers such as creatine kinase-MB and cardiac specific troponin, chest pain episodes lasting >20 minutes and ST-segment elevation >0.1 mV in more than two adjacent limb leads or >0.2 mV in more than two contiguous precordial leads or new pathologic Q waves on the surface electrocardiogram. Patients who received thrombolytic therapy or elective PCI and those treated by medical methods were excluded from this study. Non STEMI patients were not included in this study.
Study protocol
We divided the total STEMI patients into four groups according to symptom-to-balloon time (SBT) and level of hs-CRP CRP (Group I, n=2512: SBT <6 hours and hs-CRP <3 mg/L, Group II, n=660: SBT <6 hours and hs-CRP ≥3 mg/L, Group III, n=1347: SBT ≥6 hours and hs-CRP <3 mg/L, and Group IV, n=604: SBT ≥6 hours and hs-CRP ≥3 mg/L). Several studies suggested that cardiovascular disease patients with hs-CRP ≥3 mg/L are a high-risk group. Therefore, we divided groups by this level.2)12) As previously mentioned, although several studies showed a positive correlation between the level of hs-CRP and cardiovascular outcomes, some other studies failed to verify this relationship. The important difference between these studies was the duration from symptom onset to the measurement of hs-CRP. From the results of these studies, we adopted 6 hours as the criteria to divide patients into relevant groups. Moreover, because the blood level of hs-CRP ≥3 mg/L is considered a high-risk group for cardiovascular disease, we divided STEMI patients by this level of hs-CRP.
We analyzed retrospectively and compared the long-term clinical outcomes between these four groups. In order to evaluate the impact of ischemic time on the predictive value of hs-CRP, we conducted multivariate Cox-regression analyses in an early-presenting patient group (SBT <6 hours), a late-presenting patient group (SBT ≥6 hours), and total STEMI patients. Because the levels of hs-CRP were mostly measured at presentation to the hospital, SBT is nearly equal to the time from the onset of the symptoms to the measurement of hs-CRP. We defined the primary end point as the cumulative incidence of the sum of all-cause mortality and MI during a 2-year period. Additionally, we compared the incidence of cardiac death and non-cardiac death, the recurrence of MI, and the frequency of repeat PCIs between the four groups.
Statistical analysis
All analyses were performed using Statistical Package for the Social Sciences (SPSS) Version 18 (SPSS Inc., Chicago, IL, USA). Categorical baseline variables are presented as counts and percentages, and continuous variables are expressed as average value±standard deviation. Differences in baseline characteristics between STEMI patients with a high level of hs-CRP and those with a low level of hs-CRP were evaluated by a Student t-test for continuous variables and the Pearson chi-square test for categorical variables. Cumulative cardiac event-free survivals were evaluated on the Kaplan-Meier scale and compared by the log-rank method between each group. In addition, to evaluate the predicative value of hs-CRP for clinical outcomes, we used multivariate Cox-regression analysis. The co-variants for these analyses were age over 65 years, hypertension, diabetes mellitus, left ventricular ejection fraction, Killip classification, anterior wall MI, pre-Thrombolysis in Myocardial Infarction (TIMI) flow, and the use of beta-blockers and renin-angiotensine-aldosterone system (RAAS) blockers. Hazard ratios (HRs) and 95% confidence intervals were calculated, and all tests were two-tailed: p<0.05 was considered significant.
Results
Baseline characteristics
For all STEMI patients who underwent primary PCI, many baseline characteristics significantly differed between the low hs-CRP group and high hs-CRP group. The patients in the high hs-CRP group were older than those in the low hs-CRP group, and the proportion of males was lower in the high hs-CRP group. The systolic and diastolic blood pressures were lower and heart rate on presentation to the emergency room was faster among those in the high hs-CRP group. The hemodynamic state of patients was significantly different between the two groups. The left ventricular ejection fractions were lower and the percentage of patients of Killip class ≥II was higher in the high hs-CRP group. The lesion length estimated by angiography was similar between the two groups (Table 1).
Several laboratory values were also different between the high hs-CRP group and low hs-CRP group. Although the maximal levels of cardiac enzymes did not differ between the two groups, the level of N-terminal pro-brain natriuretic peptide was higher in the high hs-CRP group. The lipid profile, including total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol, were lower in the high hs-CRP group. Although the difference in blood glucose on presentation to the hospital was significant, the level of glycated hemoglobin did not differ significantly (Table 1).
Past medical history was also significantly different between these two groups. The percentage of patients with diabetes mellitus and hypertension was higher in the high hs-CRP group. However, the proportion of patients with hyperlipidemia was lower in the high hs-CRP group (Table 1).
The medications taken after primary PCI were surveyed and compared. There was no significant difference in the use of aspirin, clopidogrel, cilostazol, or statin. However, a higher percentage of patients in the low hs-CRP group took beta-blockers and RAAS blockers (Table 1).
For early presenting STEMI patients (SBT <6 hours), the differences in most baseline characteristics were similar to the differences in total STEMI patients, except in several variables. The percentages of patients who had taken beta-blockers and RAAS blockers did not significantly differ. The baseline characteristics' comparison in the late-presenting patients group is similar to that in the early-presenting STEMI patients (Table 2).
Clinical outcomes
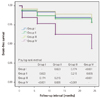
The sum of all-cause mortality and recurrence of MI was compared among Group I, Group II, Group III, and Group IV. There was a significant difference in the cardiovascular outcome among the four groups at 1, 6, 12, and 24 months (Table 3). We also evaluated the cumulative incidence of the sum of all-cause mortality and non-fatal MI and compared the event-free survival rate during 2 years. In total, for the STEMI patients who had undergone primary PCI, the patients with a lower level of hs-CRP (<3 mg/L) had a lower cumulative incidence of all-cause mortality and MI (p<0.001) than those with a higher level of hs-CRP (≥3 mg/L) (Fig. 1A). To evaluate the impact of ischemic time on the predictive value of hs-CRP, we compared the cumulative incidence of the cardiovascular event between Group I, Group II, Group III, and Group IV. Group IV had a higher cumulative incidence of cardiovascular events than the other groups (Group IV vs. Group I; p<0.001, Group IV vs. Group II; p=0.005, Group IV vs. Group III; p<0.001). However, there was no significant difference in cardiovascular events among Group I, Group II, and Group III (Fig. 2).
Detailed cardiovascular events such as cardiac death, non-cardiac death, MI, and the repeat of PCI were also compared between the four groups. The cumulative incidence of cardiac death was higher in Group IV than in the other three groups (Group IV vs. Group I; p<0.001, Group IV vs. Group II; p=0.014, Group IV vs. Group III; p<0.001). The differences in cardiac death between Group I and Group II (p=0.382), Group I and Group III (p=0.808), and Group II and Group III (p=0.329) were not significant (Fig. 3A). The incidence of non-cardiac death was higher in Group IV than in Group III (p=0.004). However, there were no significant differences in non-cardiac death in other comparisons (Fig. 3B). The recurrence rate of MI was similar between the four groups (Fig. 3C). The frequency of the repetition of PCI was higher in Group II and Group IV compared with Group I and Group III (Group II vs. Group I; p=0.001, Group II vs. Group III; p=0.001, Group IV vs. Group I; p<0.001, Group IV vs. Group III; p<0.001). However, the difference in the frequency of the repetition of PCI was not significant between Group II and Group IV (p=0.840) (Fig. 3D).
Multivariate analyses
Because many baseline characteristics that can affect clinical outcomes are significantly different between the high hs-CRP group and the low hs-CRP group, we evaluated the predictive value of hs-CRP via the Cox regression multivariate analysis. The co-variants evaluated were age over 65 years, Killip classification ≥II, anterior wall MI, hypertension, diabetes mellitus, pre-TIMI flow left ventricular ejection fraction, and the use of beta-blockers and renin-angiotensin-aldosterone system blockers. After adjusting for these covariants, hs-CRP of >3 mg/L was an independent predictor for the cumulative incidence of all-cause mortality and MI (p=0.028, HR=1.691) (Fig. 1B). This multivariate analysis showed that age over 65 years (p=0.011, HR=1.917), Killip class over II (p=0.002, HR=2.069), and the use of renin-angiotensin-aldosterone system blockers (p=0.029, HR=0.572) were also independent prognostic factors in STEMI patients.
To clarify the effect of ischemic time on the prognostic value of hs-CRP, we compared the cumulative incidence of cardiovascular events and performed a Cox regression multivariate analysis in early and late presenting patients, respectively. In early-presenting STEMI patients (Group I and Group II) with SBT <6 hours, the cumulative incidence of the sum of all-cause mortality and MI was not different (p=0.823) between the high hs-CRP group and low hs-CRP group (Fig. 4A), and the predictive value of hs-CRP for the long-term clinical outcome was not significant (p=0.381, HR=1.323) (Fig. 4B). However, the cumulative incidence of a cardiovascular event was higher in the high hs-CRP group than in the low hs-CRP group for late-presenting STEMI patients with SBT ≥6 hours (p<0.001) (Fig. 5A), and hs-CRP was an independent predictor of the long-term clinical outcome (p=0.017, HR=2.462) after adjusting for confounding variables (Fig. 5B).
Discussion
Although the high level of hs-CRP is closely associated with poor clinical outcomes among stable angina pectoris patients, there is no definite conclusion about the prognostic value of hs-CRP for long-term clinical outcomes after MI. Similarly, the predictive value of hs-CRP for long-term clinical outcomes was not conclusive for the total group of STEMI patients who were treated by primary PCI in our study. Previous studies provided a clue to a hypothesis that ischemic time plays an important role in determining the prognostic value of hs-CRP after MI. Therefore, we performed a subgroup analysis according to SBT, and the results revealed that a higher level of hs-CRP (≥3 mg/L) is an independent predictor of long-term clinical outcomes in late-presenting STEMI patients (SBT ≥6 hours). However, this is not the case for early-presenting STEMI patients (SBT <6 hours).
The long-term cardiovascular outcome of late-presenting STEMI patients with a low level of hs-CRP (Group II) was not different from that of the early-presenting patients who had undergone PCI within 6 hours from the onset of symptoms. In other words, SBT was not an important contributor to long-term clinical outcomes when the blood level of hs-CRP on admission was lower than 3 mg/L.
We defined the sum of all-cause mortality and recurrence of MI as the primary end point. Although the cumulative incidence of cardiac death was significantly higher in late-presenting STEMI patients with a higher level of hs-CRP than in other groups, the rate of non-cardiac death and recurrence rate of MI was not significantly different among the four groups. The frequency of repetition of PCI is determined by the level of hs-CRP, rather than ischemic time.
Although the pathogenic role of hs-CRP in acute coronary syndrome is not well established, some studies have suggested that the chronic inflammation of the arterial wall may play an important role in plaque rupture and following thrombus formation, and these results revealed an association between hs-CRP and the incidence of acute coronary syndrome.13-16) Hong et al.17) demonstrated that acute coronary syndrome patients with an elevated level of hs-CRP have more vulnerable plaque and a higher frequency of culprit lesions than acute coronary syndrome patients with a normal hs-CPR level. Additionally, other studies have found that hs-CRP had an adverse effect on patients with MI via the mechanism mediated by the interaction with a complement.18)19) In a rat model of MI, the results revealed that infused human CRP increased the infarction size and treatment with the CRP inhibitor decreasing the effect of human CRP.20) From these results, we can hypothesize that there is too short of a time for hs-CRP to increase the infarction size in patients with a short ischemic time. As a result, the prognostic role of hs-CRP is not significant in these patients.
There have been several other studies on the prognostic value of hs-CRP in MI. Ahmed et al.21) reported that a higher baseline hs-CRP in overweight and obese acute MI patients who were treated by PCI showed a significant association with 12-month all-cause mortality, independent of other prognostic markers. Vrsalovic et al.22) have evaluated anemia, C-reactive protein, and mean platelet volume as prognostic markers in STEMI patients, and reported that the level of C-reactive protein on admission is a significant independent predictor of short-term mortality. Mouridsen et al.23) have studied the relationship between the level of hs-CRP and the prognosis in silent MI, and reported that silent MI patients with an elevated level of hs-CRP (≥3 mg/L) had worse outcomes compared with those with a low level of hs-CRP (<3 mg/L). Raposeiras-Roubín et al.24) evaluated the prognostic value of hs-CRP, Killip class, left ventricular ejection fraction, and the Global Registry of Acute Coronary Event (GRACE) risk score, finding that a higher level of hs-CRP is a predictor of an in-hospital cardiac event in acute MI, independently of the GRACE risk score. This study also reported that a high level of hs-CRP is associated with the development of contrast-induced nephropathy. Schoos et al.25) have evaluated the higher level of hs-CRP (>2 mg/L) and type of stent as predictors of long-term prognosis. The results of this study indicate that a higher level of hs-CRP is a more important predictor in STEMI patients treated by a bare-metal stent than in those treated by a drug-eluting stent, and a bare-metal stent should then be preferred when hs-CRP <2 mg/L, and a drug-eluting stent when hs-CRP >2 mg/L, in order to decrease long-term adverse outcomes, including stent thrombosis. However, there has been no study to evaluate the impact of ischemic time on the prognostic value of hs-CRP in STEMI patients who are treated by primary PCI, as in our study.
Our study has several limitations. Although many patients were enrolled, it is a retrospective study. It is necessary to perform a prospective cohort study to evaluate the prognostic role of hs-CRP more accurately. The second limitation of our study is that many baseline characteristics are different between the high hs-CRP group and low hs-CRP group. Despite employing a multivariate analysis to overcome this shortcoming, we are not certain that all variables that can affect the clinical outcomes were adjusted completely. Additionally, to evaluate the impact of hs-CRP on the long-term outcome, it is necessary to follow-up on the level of hs-CRP. However, in our study, there was no follow-up data on the level of hs-CRP.
Despite these limitations, it is meaningful to suggest the impact of ischemic time on the prognostic role of hs-CRP for the long-term incidence of cardiovascular adverse events. From the results of this study, we assume that STEMI patients with a higher level of hs-CRP have worsened outcomes than those with a lower level of hs-CRP when the SBT is over 6 hours. However, the impact of high hs-CRP on clinical outcomes may not be significant when ischemic time is short (<6 hours). Therefore, we suggest that the treatment strategy targeting hs-CRP can be applied differently according to the ischemic time of the STEMI patient.







 XML Download
XML Download