

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The advent of P2Y12 inhibitors with antiplatelet effects has extended the use of the drug-eluting stent (DES) for occlusive coronary artery disease. Dual antiplatelet therapy (DAPT) with aspirin and clopidogrel had been considered the standard treatment in patients with acute coronary syndromes (ACSs) undergoing percutaneous coronary intervention (PCI), because DAPT has been shown to reduce the incidence of myocardial infarction (MI) or death from cardiovascular (CV) causes.1)2) Nevertheless, the incidence of ischemic events remains high among patients with ACS.3)
Clopidogrel is a pro-drug that is converted to its active metabolite principally by cytochrome (CYP) P4502C19, at which time it inhibits platelet activation by irreversibly binding the P2Y12 receptor. Genetic polymorphisms in ABCB1 and CYP2C19 may affect the absorption and metabolism, respectively, of clopidogrel, and consequently alter its pharmacodynamics. As a result, there exists high interindividual variability in the responsiveness to clopidogrel and on-treatment platelet reactivity (OPR). High OPR (HOPR) with clopidogrel use is associated with an increased risk of ischemic events in patients with ACS undergoing PCI.4-6)
Newer and more potent P2Y12 inhibitors, such as prasugrel or ticagrelor, have been shown to be superior to clopidogrel in terms of their ability to decrease ischemic events in patients with ACS. However, their benefits are limited because of increased episodes of bleeding.7)8) Personalization of antiplatelet treatment for ACS may be necessary to attain the maximum inhibition of platelet activation with a minimum risk of bleeding. The recent development of point-of-care assay kits, VerifyNow P2Y129-11) and Verigene CLO assays,12) for the assessment of platelet function and CYP2C19 polymorphisms, respectively, has enabled the immediate assignment of individualized antiplatelet treatment. However, as yet, studies using high-dose clopidogrel or prasugrel have not conclusively demonstrated a clinical benefit of the phenotype-10)13) or genotype-directed personalization of antiplatelet therapy14) based on residual platelet reactivity, or the presence of CYP2C19 loss-of-function alleles.
Therefore, the aim of this study was to investigate the feasibility of point-of-care genotypic and phenotypic testing to guide individualized antiplatelet therapy using ticagrelor in Korean patients with non-ST elevation ACS undergoing PCI. We also compared the effectiveness of genotype- and phenotype-directed antiplatelet therapy in terms of decreasing the number of patients with HOPR after 30 days.
Subjects and Methods
Trial design and study population
The present study was a single center, prospective, randomized, proof-of-concept trial. The study flow is as shown in Fig. 1. The study protocol was approved by the Ethical Review Board of Yonsei Severance Christian Hospital (Wonju, Korea). Informed consent was obtained from all participants.
Between April 10, 2012 and February 6, 2013, 65 patients aged 18-75 years were randomly assigned to genotype- or phenotype-directed treatment according to a random-number table. Patients were eligible if they had undergone PCI for non-ST-elevation ACS. Patients presenting with ST-segment elevation myocardial infarction and who had had severe left ventricular dysfunction (ejection fraction, <30%) or cardiogenic shock were excluded from the study. Other exclusion criteria were bradyarrhythmia, a history of transient ischemic or cerebrovascular attacks, a platelet count of <150000/mL, hematocrit of <30%, and a creatinine clearance rate of <30 mL/min. Patients who received a periprocedural thrombolytic agent or glycoprotein IIb-IIIa inhibitor, or who planned to use oral anticoagulants or other antiplatelet agents, such as cilostazol, were also excluded.
VerifyNow P2Y12 test
On-treatment platelet reactivity was measured using the VerifyNow P2Y12 assay (Accumetrics, San Diego, CA, USA). Blood samples were obtained 12 to 24 hours after PCI and after a 30-day follow-up period. Each sample was placed in a tube containing 3.2% citrate, and the P2Y12 reaction unit (PRU) value was assessed within 2 hours, as previously described.11) HOPR was defined as PRU value ≥230 based on previous studies involving Caucasian subjects.9)15) Although studies conducted among Korean subjects revealed that HOPR of an approximate PRU value of 270 is necessary to predict future cardiovascular events,4)16)17) we selected a PRU value of 230 as the cutoff, in order to include more patients who might benefit from phenotype-directed antiplatelet therapy.
Verigene CLO assay
All patients were screened for the CYP2C19*2, *3, or *17 allele by using the Verigene CLO assay (Nanosphere, Northbrook, IL, USA). The Verigene CLO assay is an automated sample-to-result microarray-based assay in which deoxyribonucleic acid (DNA) extracted from whole blood samples is hybridized to allele-specific probes immobilized on a glass slide. The detection of captured DNA is achieved using nanoparticle-conjugated probes that have been demonstrated to provide excellent sensitivity and that eliminate the need for a target amplification step prior to array hybridization.18) The Verigene CLO assay accurately identified homozygous and heterozygous *2 and *3 phenotypes with a specificity of 100% and a final call rate of 99.7%. The assay is automated and can yield results in approximately 3.5 hours.19)
Phenotype- versus genotype-directed antiplatelet regimen
Regardless of their prior exposure to clopidogrel, all patients received 300 mg of aspirin and 300 mg of clopidogrel before arriving at the catheterization room. A bolus of unfractionated heparin (70 U/kg) was administered immediately before coronary angiography through the introducer sheath. A second bolus of unfractionated heparin (70 U/kg) was administered immediately before the PCI. Additional heparin was administered to achieve an activated clotting time of 250-300 seconds. PCI was performed using balloon predilatation, followed by DES deployment via the transradial or transfemoral artery.
The choice regarding the specific type of DES was left to be determined by the operator's discretion. All patients were given 100 mg of aspirin daily after PCI. Patients with HOPR or who were CYP2C19 *2 or *3 carriers were also given 90 mg of ticagrelor twice daily. Patients without HOPR or who were non-carriers were given 75 mg of clopidogrel daily (Fig. 1).
Definitions and endpoints
The primary endpoint was the percentage of patients with HOPR after 30 days of DAPT. The secondary endpoints were 1) PRU, ΔPRU, percent inhibition of platelet aggregation (%IPA), and Δ%IPA, 2) the correlation between the presence of CYP2C19 *2 or *3 carriers and HOPR at the baseline, 3) the incidence of bleeding using the Bleeding Academic Research Consortium (BARC) definition,20) and 4) major adverse cardiac events (MACEs) defined as the composite of death from CV causes, non-fatal myocardial infarction, ischemia-driven target lesion revascularization, or stent thrombosis.
Statistical analysis
The proportion of patients with HOPR after 1 month of DAPT in the genotype-directed group was assumed to be 5%.14) On a ratio basis of 80%, we calculated that we needed 44 subjects per group to detect a 20% difference between the groups. The test statistic used was the two-sided Z test with pooled variance. The significance level of the test was targeted at 0.05. Assuming a dropout rate of 14%, we would therefore need 50 patients each in the genotype- and phenotype-directed groups, forming a total of 100 patients. Enrollment was ceased at 65 patients because the number of Verigene CLO assay kits was insufficient. Analysis was based on intent-to-treat or per-treatment where necessary. All continuous variables are presented as mean±SD and were analyzed using the Student's t-test. Categorical variables are presented as frequencies (percentage), and were analyzed using the chi-square test or Fisher's exact test. OPR was compared based upon the genotype using one-way analysis of variance. Post-hoc analysis was performed for any parameters found to be p<0.05. We compared platelet reactivity at the baseline and after 30 days in the genotype- and phenotype-directed groups by using the Student's t-test. The significance level was defined as p<0.05. All analyses were performed with Statistical Package for the Social Sciences (SPSS) 20.0 (SPSS Inc., Chicago, IL, USA).
Results
Of the 32 patients in the genotype-directed group, 21 CYP2C19 *2 or *3 carriers (65.6%) were administered ticagrelor and 11 CYP2C19 *2 or *3 non-carriers (34.4%) were administered clopidogrel. Of the 33 patients in the phenotype-directed group, 11 patients with HOPR (33.3%) were administered ticagrelor and 22 patients without HOPR (66.7%) were administered clopidogrel. In the genotype-directed group, there were five crossover cases from ticagrelor to clopidogrel because of dyspnea (2 patients), nasal bleeding (1 patient), petechia on the whole body (1 patient), and generalized rash (1 patient). In the phenotype-directed group, one crossover from ticagrelor to clopidogrel occurred due to dyspnea. Sixty-one patients (95.3%) had follow-up VerifyNow P2Y12 assay, 31 and 30 in the genotype- and phenotype-directed groups, respectively (Fig. 1).
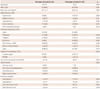
Baseline clinical and procedural characteristics between the groups are presented in Table 1. The two groups were balanced with respect to age, sex, and histories of diabetes mellitus, hypertension, hyperlipidemia, smoking, and myocardial infarction. The distribution of discharge medication use between the two groups was similar, except for the use of clopidogrel and ticagrelor. Clopidogrel was taken more frequently and ticagrelor less frequently by patients in the phenotype-guided group (clopidogrel: 34.4% vs. 66.7%, genotype vs. phenotype, p=0.009; ticagrelor: 65.6% vs. 33.3%, genotype vs. phenotype, p=0.009). The indications for PCI, left ventricular ejection fraction, and distribution of vessels stented did not differ between the groups. Procedural variables including the extent of coronary artery disease, stent number, total stent length, and mean stent diameter were also similar.
Comparison of on-treatment platelet reactivity
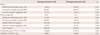
The comparison of OPR according to the personalization strategy of DAPT is as shown in Table 2. At the baseline, there were no differences in OPR, %IPA, and the percentage of patients with HOPR between the groups. OPR decreased following both genotype- and phenotype-directed therapies (242±83 vs. 109±90, p<0.001 in the genotype-directed group; 216±74 vs. 109±90, p=0.001 in the phenotype-directed group). At day 30, the percentage of patient with HOPR tended to be higher in the genotype-directed group (16.2% vs. 3.3%, p=0.086). At the 30-day follow-up, PRU and %IPA were similar between the two groups. However, ΔPRU was higher in the genotype- versus the phenotype-directed group (156±115 vs. 83±124, p=0.027). This may be due to the fact that more patients were administered ticagrelor in the genotype-directed group (51.6% vs. 33.3%, p=0.009).
On-treatment platelet reactivity according to CYP2C19 genotype
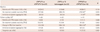
Approximately 35% of patients were heterozygous for CYP2C19 *2 or *3. 23% were homozygous for CYP2C19 *2 or were carriers of CYP2C19 *2/*3 (Table 3). Baseline OPR was higher in patients expressing CYP2C19 *2/*2 or CYP2C19 *2/*3 compared to that in patients expressing wild-type CYP2C19 *1/*1 or CYP2C19*1/*17 and in patients heterozygous for CYP2C19 *2 or *3 (280±50 vs. 214±80, p=0.004). However, no difference was found in the baseline OPR between CYP2C19 *2 or *3 non-carriers and those heterozygous for CYP2C19 *2 or *3 (217±84 vs. 209±78, p=0.880). After 30 days, ΔOPR from the baseline to follow-up was higher among patients expressing CYP2C19 *2/*2 or CYP2C19 *2/*3, corresponding with a greater percentage of patients receiving ticagrelor.
On-treatment platelet reactivity according to clopidogrel versus ticagrelor use
The number of patients with HOPR at baseline was greater in those allocated ticagrelor; however, none had HOPR after 30 days of treatment. The number of patients with HOPR did not change after 30 days of clopidogrel treatment (Table 4). Baseline OPR was significantly higher in patients slated to receive ticagrelor. After 30 days of treatment, OPR was lower (49±30 vs. 179±77, p<0.001) in patients taking ticagrelor compared to clopidogrel (Fig. 2); accordingly, ΔPRU from baseline to follow-up was higher (84±9 vs. 34±26, p<0.001) in patients given ticagrelor.
There were no MACEs in either group during the 1-month follow-up period. There were two nuisance BARC type 2 bleeding events in the genotype-directed group related to ticagrelor use.
Discussion
This was the first study that demonstrated the feasibility and effectiveness of anti-platelet therapy tailored by point-of-care genetic or platelet function testing to decrease the OPR in patients undergoing PCI. The major findings in the present study were that OPR was effectively decreased following both genotype- and phenotype-directed therapy and compared to clopidogrel, ticagrelor caused higher decrease in OPR regardless of the CYP2C19 genotype.
Heightened platelet reactivity contributes to the occurrence of ischemic events especially in certain clinical subsets such as ACS, chronic kidney disease, or diabetes mellitus. HOPR with clopidogrel treatment has also been proposed to be a predictor of ischemic CV events in patients undergoing DES implantation. To date, there is little consensus on the treatment options to overcome HOPR. Studies examining the effect of high- versus standard-dose clopidogrel have yielded discrepant findings. Mehta et al.21) noted a reduction in CV events and stent thrombosis in patients given double-dose clopidogrel, whereas Price et al.10) found no effect on CV outcomes. Price et al.10) attributed this difference to the selection only of patients with HOPR in their study, whereas Mehta et al.21) enrolled patients regardless of platelet reactivity. Although the addition of cilostazol to DAPT lowered PRU levels more than DAPT, the effect of triple versus double therapy on composite CV outcomes was inconsistent in patients undergoing PCI.22)23) The more potent antiplatelet agents, prasugrel or ticagrelor, have been shown to be superior to clopidogrel in terms of reducing CV events, but with a higher occurrence of bleeding episodes,7)8) which is associated with a higher risk of CV events.24) In the present study, ticagrelor substantially reduced OPR after 30 days. However, two patients ceased taking ticagrelor use because of nasal bleeding and the appearance of petechiae on the whole body. Because of the concern of the increased risk of bleeding, the use of parasugrel or ticagrelor is not yet widespread in Korea, even among the ACS population after PCI. Further study is therefore warranted on the effects of reduced doses of prasugrel or ticagrelor on the clinical endpoints in Korean ACS patients.
The use of point-of-care testing to tailor antiplatelet therapy according to risk stratification for bleeding and ischemia represents an ideal strategy for ACS patients. Among these tests, the VerifyNow P2Y12 assay to measure OPR is increasingly being used given the evidence suggesting an association between HOPR and CV events.9)15) However, there are several shortcomings to measuring OPR: 1) OPR is a surrogate marker only representing the inhibition of P2Y12 receptor mediated platelet activation, not whole platelet activity; 2) OPR cannot be measured in patients treated with glycoprotein IIb-IIIa inhibitors or thrombolytics; 3) PRU value varies with elapsed time following ACS or PCI;25)26) 4) the cutoff for HOPR varies according to patient ethnicity;4)16) and 5) the relationship between low OPR and bleeding events has yet to be definitively established. Moreover, trials in which antiplatelet therapy has been personalized according to the results of the VerifyNow P2Y12 assay have failed to demonstrate any improvement in outcomes.10)13)27)
By comparison, genotyping can be carried out under any clinical circumstances with no limitations with respect to timing. In previous studies, CYP2C19 *2 or *3 carriers have been shown to have higher OPR and poor clinical outcomes with clopidogrel use after PCI, compared with CYP2C19 *2 or *3 non-carriers.28) However, genotyping also has its drawbacks. Clopidgrel is a pro-drug that is converted to an active metabolite in two hepatic steps involving CYP1A2, 2C9, 2C19, 3A4/5, not only by 2C19. To date, point-of-care clopidogrel genetic testing is limited to CYP2C19 single nucleotide polymorphism;12)14) yet the CYP2C19*2 genotype only accounts for approximately 12% of the variation in the clopidogrel response.28) The feasibility of genotype-guided prasugrel use has been proven in a proof-of-concept trial,14) but the clinical benefits of genotype-guided antiplatelet therapy has yet to be demonstrated.
Although genetic testing and platelet function testing may provide additive information in selecting an antiplatelet regimen for patients undergoing PCI, their routine use is not recommended in current practice guidelines.2) Genotyping may be an improved guide for chronic antiplatelet therapy, while platelet function testing is more useful in acute settings. Nevertheless, the benefits of genotype- and phenotype-directed individualization of antiplatelet therapy to improve clinical outcomes requires validation though further randomized, controlled trials.
Limitations
A potential limitation of the present study relates to the early termination of the trial due to the unavailability of the Verigene CLO assay during the study. Furthermore, the crossover rate from ticagrelor to clopidogrel was higher in the genotype- versus the phenotype-directed group, possibly due to the higher number of patients allocated ticagrelor in the genotype-directed group. Moreover, there was no standard care control group comparing genotype- versus phenotype-directed antiplatelet therapy. Finally, our analyses were based on a single determination of the PRU value, which is subject to random measurement error and may possibly have underestimated the strength of the associations.



 XML Download
XML Download