

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stem cell therapies hold remarkable promise, particularly in the management of diseases and conditions for which there are currently limited or no treatment options.1) The ability of stem cells to self-renew and differentiate into all somatic cell types offers excellent prospects to regenerative medicine. Like all emerging technologies, however, creating new applications from an evolving knowledge base has been a slow process. In fact, there is a substantial gap between expectations and the reality of clinical stem cell application. Therefore, before clinical applications, a great deal of translational research is necessary to ensure that their therapeutic properties are both effective and safe.
Why Do We Need Translational Study in Stem Cell Treatment?
Stem cell biology is highly complex and variable. This creates challenges for regulators developing the testing necessary to ensure the quality of new technologies and therapies. There are valid concerns about the consistency of cell cultures and the genetic stability of cell lines. As an example, both human embryonic stem cells (hESCs) and induced pluripotent stem cells (iPSCs) have been shown to demonstrate genetic and phenotypic drift in long-term in vitro culture. Given that there is the potential for late tumor formation resulting from accidental mutagenesis in the creation of stem cell products, long-term monitoring of animals used in preclinical studies will be required.
Food and Drug Administration Guidance: Cellular Therapy for Cardiac Disease
The teratoma forming property of stem cells is considered a major obstacle for biomedicine by the U.S. Food and Drug Administration (FDA). The potential for tumor formation represents a concern correlated with the self-renewal of undifferentiated cells, whereas cells at other levels of maturation may also pose a risk. Namely, many stem cell-based therapies will not consist of a pure, homogeneous target cell population, which raises additional questions about risks that non-target cells may present, as well as their physiological role after administration. Additionally, the differentiation of stem cell based products that are allogeneic with respect to the recipient results in increased immunologic incompatibility, due to the expression of foreign non-self antigens. In addition, the death of large proportions of the transplanted cell population, not unique to stem cells, may constitute further risk.2) To determine whether it is reasonable to grant permission for a clinical trial to proceed, the FDA evaluates potential risk based on results derived from the analytical assessment of product characteristics, as well as preclinical proof-of-concept and safety testing, which, collectively, are considered within the context of a proposed clinical study.3)
What Types of Animal Model Might Work in Stem Cell Therapy?
Small animals (mice, etc.) can provide information regarding the ability of the human cellular product to target the myocardium, as well as offering insight into potential safety issues related to the administered cells. These models can be used to study the potential for cellular products to survive and differentiate in the myocardium following infarction. However, they do not let themselves to use in any sensitive evaluation of overall cardiac function or unfavorable results related to the administration of cellular products, due to restrictions of anatomy and physiology related mainly to body size.
Large animals (swine, etc.) can provide information on the safety and activity of cellular products and delivery systems. As well, these models can be used to address issues such as cell numbers, volume, rate of injection, and the optimal location for product administration. These data cannot be generated using small animal models due to the inability to directly test catheters for clinical use and the limited ability to monitor cardiac function. The use of a sustainable and reproducible large animal model is a crucial step for various researchers to obtain FDA Investigational New Drug approval.
What Types of Heart Disease Have Been Indicated for Stem Cell Therapy?
Over the past decade, major advances in stem cell biology have created great promise for regenerative medicine. In vivo transplanted stem cells can proliferate and differentiate into cardiomyocytes, endothelial cells, or smooth muscle cells (Fig. 1). This concept of stem cell transfer for enhancing cardiac repair has raised new therapeutic prospects. Although the underlying mechanisms remain poor, promising results have been reported in early preclinical studies. Despite ongoing controversies, clinical trials have shown a reassuring safety profile and suggest functional benefits. A number of clinical trials of stem cell therapy for cardiac repair have been registered with clinicaltrials.gov. These are listed in Table 1.
Stem cell therapy in acute myocardial infarction
The majority of the studies have used intracoronary delivery following successful stenting of the infarct-related artery. Improvements in the left ventricular systolic function and the reduction in the size of scar tissue and cardiac volume have been referred to as the surrogate markers used to assess the efficacy of cell therapy.
Many studies showed improvements in ejection fraction, wall motion abnormalities, volume reduction, and reduced infarction size. In contrast, some trials did not demonstrate any benefits. The reasons for the inconsistent findings remain unclear, but the possibilities comprise differences in the cell numbers, timing, evaluation methods, and follow up periods. Past clinical trials are summarized in Table 2.4-9)
Stem cell therapy in chronic ischaemic cardiomyopathy
Initially, stem cell implantation was investigated in patients undergoing open-heart surgery. Mostly, the employment of direct intramyocardial injection methods has been used. Most recently, percutaneous transcatheter intramyocardial injection was introduced. Stem cell transplantation has been assessed in regional contralility, New York Heart Association functional class, quality of life, and evidence of reverse ventricular remodeling. Stem Cell Infusion in Patients with Ischemic CardiOmyopathy (SCIPIO) was the first trial using autologous cardiac progenitor cells in heart failure. In this first trial, results demonstrated an improvement in ejection fraction, heart failure score, and reduced infarction size.10) However, some trials did not produce any significant results.11)12)
How Do We Develop an Experimental Animal Model?
Swine are superior large animal models for studies of acute myocardial infarction (MI) and ischemic cardiomyopathy (ICM), because the coronary artery anatomy, size, structure, and distribution make them suitable for preclinical cardiovascular research. As with the human anatomy, the porcine left anterior descending artery (LAD) provides approximately half of the blood supply to the left ventricle (LV), and its occlusion creates an MI that is similar in size and distribution to that occurring in humans as a result of LAD occlusion (Fig. 2). This is commonly used as a model of human cardiovascular disease.13-17) Although the left circumflex coronary artery occlusion technique has its benefits, such as lower procedural mortality, LAD occlusion is the preferred model for preclinical studies, considering that this is where the majority of human MI occurs.18) Moreover, the pattern of remodeling as a result of the MI closely resembles that occurring in humans.19) These similarities make the swine model highly appropriate for translational research, as the equipment and procedural techniques used to quantify these variables are analogous to those used in humans.
Acute myocardial infarction model
To establish a reproducible acute MI model, a percutaneous balloon catheter is used to occlude blood flow at the distal part of the first diagonal branch in the LAD. By restoring the blood flow of the first diagonal branch, some territory of the LV muscle can be saved. Accordingly, a portion of survived myocardium shows a border zone to the infracted myocardium.
Occlusion of the coronary artery can provide a predictable and reproducible MI model of anteroapical, lateral, and septal myocardium. The mechanism of the acute MI model results from reperfusion injury. After balloon occlusion, the myocardium is completely reperfused to mimic acute MI. According to protocols, by modifying occlusion time and location, an animal model could be provided.20)21)
Chronic ischemic cardiomyopathy model
To make a chronic model of ICM, stenosis or an occlusion model with significant depression of the LV are required. A chronic ICM model using a plastic occlude on the LAD has developed with low mortality rates and easy reproducibility. A plastic occluder of a fixed diameter and an 18-gauge copper wire were deployed around the proximal segment of the LAD coronary artery and fixed loosely with a cotton umbilical tape. A plastic occlude with a fixed diameter of 1.0 mm, fitted with an 18-gauge copper wire, was placed on the proximal LAD.15) Oral administration of dual anti-platelet agents were followed by the operation for 10 days.
What Types of Stem Cells Have Been Applied and What about the Future?
Various stem cell populations exist, derived from both embryonic and adult human tissue sources. The most frequently studied stem cell populations in cardiac disease include embryonic stem cells, bone marrow-derived stem cells, tissue-specific stem cells, and, most recently, iPSCs. Each one has its own particular characteristics. According to current experiments, the findings are summarized in Table 3.22)
The optimal cell type for ischemic heart disease remains a controversial subject of debate. Previous studies have examined various cell types.23-25) Probably, different stem cell types will be considered in different heart disease types. The ideal cell type should meet the following standards: it must be safe, effective, able to regenerate healthy and functional cardiac muscle, easy to harvest, have no immune reaction, and it must not raise ethnical issues.
Currently, the major type of different stem cells used for basic and clinical studies in ischemic heart disease is mesenchymal stem cell, which have tremendous clinical potential due to their high expansion ratio and ability to be used for allogeneic transplantation.26)
How Can Stem Cells Be Delivered to Animals?
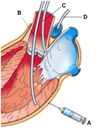
A variety of methods have been used to deliver stem cells to the heart. These methods have included local intramyocardial injection, epicardial injection, intravenous injection, and intracoronary injection related to the infarct zone (Fig. 3). There are no definitive answers provided by these methods, but direct cell delivery into the injured heart is considered the most promising method of delivery. In large animal models, several studies have confirmed the safety and feasibility of direct injection methods.27-29)
Intracoronary infusion
Stem cells are injected into coronary circulation. In this way, we can deliver a higher concentration of SCs to the heart. This approach was first introduced in 2001 in a feasibility study of stem cell transplantation after primary percutaneous coronary intervention for acute MI. Since that trial, the majority of stem cell studies have been performed using this method.30)
This approach is less invasive, safe, and quite feasible. Because intracoronary infusion must use an opened occluded coronary artery, however, this technique is limited to the acute MI model. Besides, this approach poses the risk of coronary embolism and it is difficult to deliver to poor arterial supply. However, this selective intracoronary infusion approach remains the predominant stem cell delivery route. This intracoronary infusion has been verified as a feasible, safe technique and has demonstrated improvements in cardiac function as well as reductions in infarct size following intracoronary infusion.
Direct epicardial injection
By needle, stem cells are directly delivered into the myocardium. This epicardial procedure has been the most direct, precise, and accurate approach for injecting stem cells into an infracted region of the heart. The location can be identified preoperatively using imaging modalities, during surgery, by empirical observation.31) Direct intramyocardial injection can typically be conducted either during open heart surgery like coronary artery bypass graft32) or as a separate procedure performed without cardiac arrest via a lateral minithoracotomy.33) It offers the distinct advantage of targeting localized myocardium without perturbing any surrounding tissue and vasculature. In contrast to the intracoronary approach, myocardial injection enables stem cells to be delivered to an infracted area with a limited blood supply. Thereby, it circumvents the need to address complex issues such as mobilization of the transplanted cells. In addition, stem cells can be injected into the border zone of the infarction. Furthermore, there is no risk of coronary embolism. Therefore, an epicardial injection is performed in conjunction with open-heart surgery or left ventricular assistive device implantation,34)35) even if it was the most widely used method in preclinical research in small animals at first.
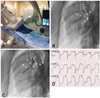
Transendocardial injection
This direct injection can be carried out percutaneously and less invasively than an epicardial injection.36) Through the coronary vessel, a percutaneous catheter is entered into the left ventricular cavity. However, specialized catheters are needed for this method. With the introduction of new catheters and imaging modalities, physicians and scientists are now able to apply intramyocardial injections as a potential cellular therapy (Fig. 4). This method was first implemented and validated in a swine model by Fuchs et al.37) Since then, many clinical studies have been published with largely positive indications of its efficacy. No observations of any significant adverse complications have been made so far. However, this approach poses the potential risk of inducing fatal ventricular arrhythmia. To date, the equipment required is expensive and not widely available. With the continuous and rapid development in catheterization techniques and imaging devices, transendocardial injection appears to be a very viable, feasible, and safe approach for further investigation in the future, pending the results of current clinical trials.
Current Status and Trends of Stem Cell Clinical Trials around the World
Since those initial reports, numerous additional clinical stem cell trials have been conducted in the treatment of cardiac disease. Currently, iPSCs are not being conducted as clinical trials, but a hESCs trial commenced in October 2010 by Geron for spinal cord injuries. Unfortunately, this trial was halted in November 2011 after use in only four trial subjects. As of 2013, clinical trials for cardiovascular disease numbered 236 studies worldwide: 75% targeted the heart and 25% the peripheral vascular system. Almost all of these trials involved messenchymal stem cells, the mobilization of hematopoietic stem cells, other purified bone marrow-derived stem cells, or endothelial progenitor cells for regenerative and supportive purposes (Fig. 5).
Summary
In translational research, stem cell study is one of the most actively proceeding field. With the help of these preclinical research efforts, at present, new and exciting stem cell therapies are already being applied in clinical applications, as seen in the SCIPIO, Prospective Randomized Study of Mesenchymal Stem Cell Therapy in Patients Undergoing Cardiac Surgery (PROMETHEUS), the PercutaneOus StEm Cell Injection Delivery Effects on Neomyogenesis pilot study (POSEIDON), dilated cardiomyopathy (POSEIDON-DCM), and Transendocardial Autologous Cells in Ischemic Heart Failure Trial (TACHFT) trials.10)38-41)
Conclusion
The rapid progress of stem cell research has allowed for the almost simultaneous development of preclinical and clinical studies. However, questions still remain unanswered regarding the optimal type, dosing, timing, and delivery of stem cells. To establish convincing stem cell therapy, ongoing efforts in the exchange of knowledge from the bench to the bedside are required.






 XML Download
XML Download