

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The time-to-reperfusion in the setting of ST-segment elevation myocardial infarction (STEMI) is an important predictor of clinical events and outcomes.1)2) Therefore, rapid diagnosis of STEMI is essential for an appropriate management of patients.3)4) However, the decision to provide immediate reperfusion therapy to patients presenting with chest pain and ST-segment elevation may not be simple since STEMI is not the only cause of ST-segment elevation on electrocardiography (ECG).5-16) False-positive catheterization laboratory activation is a significant concern because of procedural risks to the patient and burdens on financial resources.17) Although limited data is available on the prevalence of false-positive catheterization laboratory activation in patients undergoing percutaneous coronary intervention (PCI) for suspected STEMI,17)18) we predicted that the causes of false-positive catheterization activation may differ in Korea compared with the reports from Western countries.17)18) The objective of the present was to determine the prevalence, etiologies and predictors of false-positive diagnosis of STEMI and subsequent inappropriate catheterization laboratory activation in patients with presumptive diagnosis of STEMI.
Subjects and Methods
Study population
Four hundred fifty-five consecutive patients with presumptive diagnosis of STEMI who underwent emergency coronary angiography for primary PCI at Kyungpook National University Hospital, Daegu, Korea between August 2008 and November 2010 were included. All patients except one (n=454, 99.8%) were ethnic Korean and presented within the first 12 hours after symptom onset with ST-segment elevation or new left bundle branch block (LBBB) on ECG were considered eligible for primary PCI. Patients with symptom onset >12 hours were also included if they were symptomatic on arrival. The decision to activate the catheterization laboratory for primary PCI was made by the physician in the Department of Internal Medicine and communicated by face-to-face notification during on-duty hours and by the emergency physician via a phone call to the on-call interventional cardiologist during off-duty hours, who would in turn activate the entire staff involved in primary PCI.
Data analysis and definition
ST-segment elevation was defined as J-point elevations in ≥2 leads, with a cutoff of ≥0.2 mV in leads V 1, V 2, or V 3 and ≥0.1 mV in other leads. In patients with LBBB, ST-segment elevation was defined as ST-segment elevation ≥0.5 mV and discordant with QRS complex.19) ST-segment elevation was assessed relative to the RR segment. ST-segment depression in the following leads was identified as reciprocal ST-segment change: leads I, aVL in inferior STEMI, leads II, III, aVF in anterior STEMI and III, aVF in lateral STEMI.20) All ECGs were reviewed by Y Cho and MH Bae at our hospital. Each 12-lead ECG was separately reviewed for the presence or absence of ST-segment elevation, Q wave, reciprocal changes, left ventricular hypertrophy (LVH), LBBB and right bundle branch block (RBBB). The height of maximal ST-segment elevation and the number of leads with ST-segment elevation were also recorded. The cardiac troponin I (cTnI) levels were measured on admission and every 6 hours after to detect the presence of myocardial injury using an enzyme immunoassay based on the sandwich principle kit (Dimension; Dade Behring, USA); the lower detection limit of this assay was 0.04 ng/mL. Elevated cardiac biomarker levels were defined as maximal values of cTnI that exceeded the decision limit (99th percentile of the values for a reference control group) on at least one occasion. A culprit coronary lesion was identified if a coronary lesion corresponding to the electrocardiographic changes was found. False-positive catheterization laboratory activation for STEMI was defined as the absence of a culprit coronary artery in patients who underwent emergency coronary angiography for planned primary PCI. Myocarditis was defined by flu-like signs and symptoms, typical ECG findings of pericarditis, elevations of cTnI levels and normal coronary artery by angiography.21) A final diagnosis of stress-induced cardiomyopathy was based on characteristic 2-dimensional (D) echocardiographic wall motion abnormalities in the mid and distal left ventricle and associated psychological stress preceding the cardiac event.22) Coronary spasm was defined if culprit spastic vessel was relieved by intracoronary nitroglycerin injection or if the result of a ergonovine test was positive; total or near total occlusion of culprit vessel with concurrent chest pain and/or ST-segment elevation.23) LVH was based on the definitions of Sokolow and Lyon.24) Previous myocardial infarction (MI) with persistent ST-segment elevation was defined by history of a Q-wave MI with ST-segment elevation that was either demonstrated on a previous ECG or did not demonstrate ST-segment evolutionary changes.17) Early repolarization was identified in patients with negative cTnI results and the following ECG findings: elevated concave ST-segment, located commonly in the precordial leads (most conspicuous in leads V 1-3), tall peaked T waves, a slur on the R wave.5)6) Clinical, laboratory, 2-D echocardiographic, angiographic, and outcome data for all patients who had the diagnosis of presumptive STEMI were collected. Two-D echocardiography was performed within 24 hours after arrival in most cases.
Statistical analysis
Data are presented as mean±standard deviation for continuous variables and percentages for categorical variables. Patients were categorized into a STEMI group and a false-positive STEMI group. Comparisons were made using the Student's t-test for continuous variables and the chi-square test for categorical variables. The p were 2-sided, and p<0.05 was considered significant. Multiple logistic regression analysis was used to determine independent predictors of false-positive catheterization laboratory activation for STEMI, and adjusted for baseline confounding characteristics with p<0.05 in univariate analysis. Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS)® version 15.0 for Windows® (SPSS Inc., Chicago, IL, USA).
Results
Prevalence of false-positive catheterization laboratory activation
Four hundred fifty-five consecutive patients who underwent emergency coronary angiography for primary PCI with presumptive diagnosis of STEMI were enrolled in this study. Four hundred twenty-one patients (92.5%) had identifiable culprit lesion(s) in coronary arteries responsible for the presumptive diagnosis of STEMI, and classified as true-positive for catheterization laboratory activation in those patients. The frequencies of anterior and inferior STEMI were 45.3% and 40.8%, respectively. Thirty-four patients (7.5%) had either normal coronary arteries or significant coronary lesions which were not responsible for the suspected STEMI leading to the classification of false-positive for catheterization laboratory activation and cardiac biomarker results were negative in 18 patients.
Patient characteristics
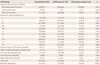
The baseline patient characteristics are shown in Table 1. The mean age was 62±13 years and 345 patients (75.8%) were men. There was a higher proportion of dyslipidemia (p=0.006) in the STEMI group. The false-positive group had a significantly longer symptomto-door time (p=0.048) and significantly higher proportion of symptom-to-door time >12 hours (p=0.015) compared with the STEMI group. Two hundred eighty-three patients (62.2%) were referred from regional medical centers with no primary PCI capability, and presentation to a district hospital without primary PCI capability was not associated with false-positive catheterization laboratory activation (p=0.123). Among the 264 patients referred with their official transfer note, 36 patients (13.6%) had been diagnoses with conditions other than STEMI, which were not associated with false-positive catheterization laboratory activation (p=0.465). The presenting symptoms in patients with the presumptive diagnosis of STEMI included chest pain in most patients (n=427; 93.8%), epigastric pain (n=7), dyspnea (n=5), mental status change (n=5), and syncope (n=3). Presenting symptoms other than chest pain were associated with false-positive catheterization laboratory activation (p=0.048). The in-hospital mortality was not different between the STEMI group and the false-positive STEMI group (p=1.000). During the 6-month follow-up period after the index admission, there were four all cause deaths (3 cardiac and 1 non-cardiac death) in the STEMI group. However, there was no all cause deaths in the false-positive STEMI group during 6-month follow-up period.
Electrocardiography parameters of false-positive catheterization laboratory activation
Comparisons of ECG parameters are listed in Table 2. Compared to the STEMI group, the false-positive group had a significantly higher proportion of left anterior descending artery (LAD, p=0.034), and a lower proportion of right coronary artery (p=0.018) as suspected ECG territory for STEMI. Proportions of ST-segment elevation in leads III (p=0.003) or aVF (p=0.003) were significantly higher in the STEMI group and the proportion of ST-segment elevation in lead V 3 (p=0.006) was significantly higher in the false-positive STEMI group. The number of leads with ST-segment elevation (p=0.389) and the height of maximal ST-segment elevation (p=0.534) were not different between the two groups. LVH (27.3% vs. 14.0%, p=0.041) and LBBB (5.9% vs. 0.5%, p=0.030) were significantly more prevalent in the false-positive STEMI group than in the STEMI group. However, Q waves (21.2% vs. 50.5%, p=0.005) and reciprocal changes (24.2% vs. 74.7%, p<0.001) were significantly less common in the false-positive STEMI group than in the STEMI group. Among the STEMI group, reciprocal changes were significantly more common in patients with inferior STEMI than in patients with anterior STEMI (95.3% vs. 53.2%, p<0.001).
Etiologies and complications of false-positive catheterization laboratory activation
The causes of false-positive catheterization laboratory activation among the 34 patients are listed in Table 3. Among these patients, 16 (3.5%) had positive and 18 (4.0%) had negative cTnI results. Common causes of false-positive diagnosis were coronary spasm in 10, LVH in 5, myocarditis in 4, early repolarization in 3, and previous MI and stress-induced cardiomyopathy in 2 each. Aortic dissection, unstable angina, pericarditis, mediastinitis, pericardial fat necrosis, cholecystitis, LBBB and RBBB on ECG were found to be uncommon causes of false-positive catheterization laboratory activation.
Predictors of false-positive catheterization laboratory activation
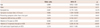
Multivariate logistic regression analysis as described in Table 4 indicated that symptom-to-door time >12 hours {odds ratio (OR) 4.995, 95% confidence interval (CI) 1.384-18.030, p=0.014}, presenting symptom other than chest pain (OR 7.709, 95% CI 1.255-39.922, p=0.027), absence of Q wave (OR 9.082, 95% CI 2.631-31.351, p<0.001) and absence of reciprocal changes on ECG (OR 17.987, 95% CI 5.295-61.106, p<0.001) were independent predictors of false-positive catheterization laboratory activation after adjusting for age, gender, dyslipidemia, suspicious LAD territory and LVH on ECG.
Discussion
The primary finding of the present study was the 7.5% prevalence of false-positive diagnosis of STEMI and subsequent inappropriate catheterization laboratory activation with predominant causes of coronary spasm, LVH, and myocarditis. Among ECG parameters, the absence of Q wave and reciprocal changes were important independent predictors of false-positive catheterization laboratory activation.
Door-to-balloon time in the setting of STEMI is an important predictor of clinical events and outcomes.1)2) Rapid interpretation of ST-segment elevation on ECG is essential for decreasing door-to-balloon time in patients with suspected STEMI.3)4) However, the decision to provide immediate reperfusion therapy to patients presenting with chest pain and ST-segment elevation is not always easy to make because ST-segment elevation in conditions other than STEMI is not rare.5-16) The common causes of ST-segment elevation include early repolarization pattern, normal male-pattern ST-changes, LVH, LBBB, pericarditis and ventricular aneurysm.5-9) Acute myocarditis, Brugada syndrome, stress-induced cardiomyopathy, aortic dissection, myocardial bridge and coronary spasm are also known rare causes of ST-segment elevation that are not rarely mistaken for MI.10-16) In this study, the etiologies of false-positive catheterization laboratory activation were different from those documented in several studies from Western countries.14)17)18) The proportion of coronary spasm (29.4% vs. 1-7%) was significantly higher and the proportion of pericarditis (2.9% vs. 11-83%) was lower in this study. The proportions of LVH, early repolarization, stress-induced cardiomyopathy and myocarditis were not different.14)17)18) It is well known that the prevalence of coronary spasm appears to be higher in the far East than in the West,15) and this racial difference is most likely one explanation of the higher proportion of coronary spasm in this study. Brugada syndrome, which is known to be more common in Asians than in Caucasians,11) and myocardial bridge was not a cause of falsepositive STEMI diagnosis in the present study.
In Korea, the government urges every hospital performing primary PCI to reduce the door-to-balloon time in cases of STEMI treated with primary PCI to less than 90 minutes, ideally less than 60 minutes, and achievement of shorter mean door-to-balloon time became one of the most important factors in grading hospitals and reimbursement in the management of patients with STEMI. However, as the interhospital transport system for STEMI patients has not been firmly established in most parts of Korea, patient data such as ECG are usually not available until the arrival of the patient. Relatively higher proportion of coronary spasm among cases of falsepositive STEMI in this study might be associated with no proper interhospital referral system in place.
In the present study, symptom-to-door time >12 hours was an independent predictor of false-positive catheterization laboratory activation. Also pathologic Q wave, associated with time delay and infarct size in the course of acute MI,25) had significance. A previous study9) reported that half the cases of false-positive diagnosis of STEMI were in patients with previous MI and in these patients, the distinction between ST-segment changes due to old and new MI were very difficult. However, in the present study, Q waves were more prevalent in the STEMI group than in the false-positive group, implying their clinical significance in the diagnosis of STEMI. Our study showed that the absence of reciprocal changes was the most important independent predictor of false-positive diagnosis of STEMI. Reciprocal changes were reported to be as more frequent in patients with inferior STEMI compared with anterior STEMI26)27) as observed in this study (95.3% vs. 53.2%, p<0.001). Among the patients with anterior STEMI, patients with a LAD artery lesion proximal to the first diagonal branch and a wrapped LAD artery, or with a LAD artery lesion distal to the diagonal branch and a nonwrapped LAD artery do not have a reciprocal change.20) Despite the limitations in anterior STEMI, the presence of reciprocal changes on ECG is very useful for the rapid and correct diagnosis of STEMI in patients with a suspected inferior STEMI, although it lacks specificity.
There are several limitations in this study. First, this was a single-center observational study with a relatively small sample size. Second, an overemphasis on false-positive STEMI may induce under diagnosis of true STEMI potentially leading to fatal prognosis of patients. However, the rate of false-negative diagnosis of STEMI was not evaluated since this study focused on false-positive diagnosis of STEMI.
In conclusion, false-positive diagnosis of STEMI and subsequent inappropriate catheterization laboratory activation were not rare. Prudent ECG interpretation and consideration of ST-segment elevation on ECG in conditions other than STEMI may reduce inappropriate catheterization laboratory activation.


 XML Download
XML Download