

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary artery fistula (CAF) is an abnormal communication between an epicardial coronary artery and a cardiac chamber, major vessel or other vascular structures. CAF is not common but is clinically important in adulthood due to an increased risk of complications, such as heart failure, myocardial ischemia, arrhythmias, infective endocarditis and rupture. The echocardiography, coronary angiography and multi-detector computed tomography are the most frequently used diagnostic methods. Current treatment options include careful observation, surgical ligation with or without bypass of the involved coronary artery and trans-catheter embolization. We present a case in which a dilated left main trunk (LMT) and proximal circumflex coronary artery are connected with a dilated coronary sinus (CS). Furthermore, another feature of this case is persistent left superior vena cava (PLSVC) and two other arteriovenous fistulae. The coronary fistula was managed conservatively.
Case
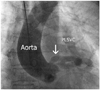
A 71-year-old woman without significant medical and family history visited the local hospital with exertional dyspnea and palpitations for 1 month. She had transferred to our hospital due to an unusual finding on transthoracic echocardiography (TTE), which was suspicious of CAF. On physical examination, the blood pressure was 125/80 mm Hg and chest auscultation revealed a continuous murmur over the left anterior chest, which was graded as Levine 2/VI. Chest radiography showed an increased cardiothoracic ratio and electrocardiography (ECG) showed atrial fibrillation. The heart rate was 75 beats/min. On TTE, a dilated LMT connecting to a dilated vessel was seen. Turbulent flow was observed on color Doppler behind the aortic root; moreover, a dilated CS with a PLSVC was identified by injection of agitated saline (Fig. 1). Also, TTE revealed a dilation of both the atrium and the pulmonary artery. A provisional diagnosis of aneurysm of the LMT with CAF and PLSVC was made. The patient underwent conventional coronary artery angiography, which showed a giant aneurysm of the LMT (9.05 mm) with tortuous and aneurysmal CAF (Fig. 2). Also, a right conal branch connecting to the pulmonary trunk was revealed. The right heart catheterization documented a pulmonary to the systemic blood flow ratio (Qp/Qs) of 1.72, which indicated the presence of a significant left to the right shunt. As the distal drainage site was not well identified on the conventional coronary artery angiography, ECG-gated multi-detector computed tomogram angiography (CTA, Brilliance 64 CT scanner, Philips Medical Systems, Cleveland, OH, USA) was performed. The CTA clearly demonstrated an aneurysmal change of the LMT, the proximal segment of the left circumflex artery and the obtuse marginal branch that connected to the dilated CS. The CTA showed that the distal segment of the left circumflex artery and the left bronchial artery were connected to the CS. Also, the CTA revealed the presence of a fistulous connection between the right conal branch and the pulmonary trunk, as well as the sinoatrial nodal artery originating from the LMT connected to the CS through the tortuous vessel (Fig. 3). CTA revealed a PLSVC. However, the connection between the two superior vena cavas (SVCs) was not observed; neither stenosis nor occlusion of CS ostium was seen. Due to multiple fistulae, severe dilation of the native coronary artery, extreme fistula tortuosity and difficulty in cannulating the distal fistula, the patient was considered not to be a candidate for percutaneous trans-catheter closure (TCC) and was recommended for surgical ligation of the fistula by a cardiothoracic surgeon. However, the patient refused surgery and requested to be managed conservatively. Her advanced age and the risks of surgical ligation were taken into consideration, and medications such as aspirin, ramipril and digoxin were prescribed for management of the atrial fibrillation. She was asymptomatic at the 1-year follow-up.
Discussion
The overall incidence of CAF is presumed to be about 0.002%, and it comprises 0.31% of all congenital heart defects. Also, the incidence has been reported in about 2% of coronary angiographies.1) No definite pathogenetic explanation has been described for CAF. It has been postulated that the lack of such explanation may be due to failure of obliteration of the intra-myocardial trabecular sinusoids with anomalous development of the intra-trabecular spaces, through which blood is supplied to the myocardium during intrauterine life.2) Although the cause of occurrence is mostly congenital, iatrogenic fistula has been reported, though its occurrence is rare. According to previous studies, 50% of CAF originate from the right coronary artery, about 42% from the left coronary artery and 5% from both of them. Very rarely does it originate from the left circumflex coronary artery (LCX). Forty one percent drain into the right ventricle, 26% into the right atrium, 17% into the pulmonary artery, 7% into the CS, 3% into the left ventricle and 1% into the SVC.1)3) PLSVC should be suspected whenever a dilated CS is discovered. Also, almost 40% of patients with PLSVC might have a variety of associated other congenital malformations of the heart and great vessels. Therefore, further examination is required. In this case, we found a dilated LMT and LCX fistula, which drained into the CS with a PLSVC. In addition, two other fistulae were also observed. This combination is very rare and we could not find any previous report of it on review of the literature.
Although coronary angiography is the gold standard diagnostic test for detection of CAF, CTA may be an alternative test, particularly for CAF coursing between vascular structures and for directing origin and the drainage site of fistula through its excellent spatial resolution and ability to show the relationship of anatomic structures. The diagnosis of the CAF in our patient was primarily conducted by coronary angiography. However, the modality failed to visualize the exact termination of the fistula. The use of CTA confirmed its termination into the CS. Likewise, a multifaceted approach is required for an accurate diagnosis and therapeutic plan when abnormal vessel is found.
The management of CAF is still a controversial issue (particularly in asymptomatic patients).4)5) There are no consistent guidelines for treatment as these fistulas have variable sizes and anatomical variants. However, it is well established that ischemic symptoms, significant shunt (Qp/Qs>1.5 regardless of symptoms), and the associated aneurysmal dilatation are indications for treatment.6-8) Therefore, due to the patient's complaints of exertional dyspnea and a Qp/Qs>1.5, our patient was deemed to be in need of treatment. Two treatment modalities are available for fistula closure: surgical or percutaneous TCC. The first successful surgical closure was reported by Björk and Carfoord in 1947,1)9) whereas the first therapeutic embolization was performed in 1974 by Zuberbuhler et al.10) The treatment modality that was used depends on the age of the patient, the morphology and the size of the fistula, as well as the presence or absence of an associated heart disease.6) Surgical closure by epicardial and endocardial ligation is the gold standard in the treatment of CAF, and remains as a safe and effective procedure with good reported rates of success.8) Since the use of advanced interventional devices, there has been an increase in the TCC treatment of CAF in recent years.11) Because TCC of CAF is associated with a much shorter recovery time and avoids scarring, it is considered as the procedure of choice when fistula closure is indicated.12) Armsby et al.13) recently showed that TCC of CAF is an acceptable and efficacious alternative to surgery in most patients.14) Coil embolization is most frequently used with successful results when there is an absence of multiple fistulas and no large branch vessel, and when there is a single narrow draining site, with safe access to the coronary artery supplying the fistula.15) Specifically, patients with large fistulae, multiple openings or aneurysmal dilatation of significant size may not be optimal candidates for TCC. Complications with TCC include proximal or distal coil migration, thrombosis of parent epicardial vessel, distal undersizing of the coil, resulting in a high shunt flow, coronary artery spasm, fistula dissection, dysrhythmias and infective endocarditis.7)
In this patient, the correlation between the symptoms and the CAFs could not be found. Nevertheless, because a significant shunt and aneurysmal dilatation were confirmed, prevention for complication was able to be considered. In addition, the patient was in good performance status in spite of her age. Because the fistula was extremely tortuous, and there was difficulty in cannulating the distal fistula, our patient was not considered a candidate for TCC, and thus, surgical ligation of fistula was recommended by the cardiothoracic surgeon. However, the patient refused surgery and requested to be managed conservatively. She was asymptomatic at the 1-year follow-up.
In summary, we report a case of a 71-year-old woman with a rare combination of dilated LMT and circumflex coronary artery with a fistula terminating into the dilated CS associated with a PLSVC. Although most CAFs enlarge progressively and warrant repair, by either trans-catheter or surgical techniques, our patient was managed conservatively at her request.


 XML Download
XML Download