

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intravascular ultrasound (IVUS) has been known to be a useful tool during coronary angiography (CAG) and percutaneous coronary intervention (PCI).1-6) It helps us to see directly the coronary vessel wall including atheroma, while angiography shows us only luminography. Moreover, after stent deployment, IVUS can be used to confirm whether there is good apposition between the vessel wall and the stent. Suboptimal deployment may give rise to subacute thrombosis or restenosis in both bare-metal stents (BMS) and drug-eluting stents (DES).7-11) Based on the information obtained by IVUS, we could repeat inflation with a balloon at higher pressure, resulting in improved stent apposition and a wider luminal cross section area.
Previous studies have compared clinical outcomes of PCI with and without IVUS-guidance.12-16) In the real world practice, however, coronary interventionists usually use IVUS 'selectively' only when it is judged to be needed. There has not been a study comparing clinical and angiographic outcomes between the two different strategies: 'routine' IVUS-guidance vs. 'selective' IVUS-guidance in the DES era. The purpose of this study was to determine whether the selective use of IVUS is comparable to the routine use in terms of angiographic as well as clinical outcomes.
Subjects and Methods
Study design
This was a single-center retrospective analysis of native coronary vessel DES implantations from August 2003 through September 2006 in the DES registry of Seoul National University Hospital. The study population consisted of patients with coronary artery disease who underwent elective and emergency coronary artery stenting of the native coronary vessel with a paclitaxel-eluting stent to exclude the bias coming from the use of different stents. The study population was divided into 2 groups: routinely IVUS-guided vs. selectively IVUS-guided. The routinely IVUS-guided group consisted of patients in whom stent implantation was performed with IVUS guidance as far as it was possible to perform IVUS examination even if angiographic findings showed good appearance. In contrast, the selectively IVUS-guided group was comprised of patients in whom IVUS was used after being judged to be needed by the operators. Judgements were made when the operators were not confident whether malapposition, edge tear or underexpansion was present or not. Patients were followed up for 1-year for mortality, myocardial infarction (MI), stent thrombosis, target lesion revascularization (TLR) and target vessel revascularization (TVR). For patients who underwent more than one procedure, the first intervention was used for the analysis. The local institutional review board approved this study.
Clinical outcomes
Clinical data at baseline and follow-up were obtained from outpatient medical records or telephone interviews. The major adverse cardiac event (MACE) of this study was the composite of death, MI, stent thrombosis and TVR including TLR. MI was defined as new significant electrocardiographic Q waves or a creatinine kinase-MB isoenzyme level >3 times the upper limit of normal.
Quantitative coronary angiography
Coronary angiograms taken at baseline, at completion of stenting, and at follow-up were analyzed in our angiographic core laboratory (Seoul National University Hospital, Seoul, Korea).
Intravascular ultrasound imaging
The timing of IVUS imaging was decided by the operator (i.e., preimplantation or postimplantation or both). The vessel including the stented area was imaged with a mechanically rotated IVUS transducer. The imaging catheter was withdrawn with an automatic pull-back device at 0.5 mm/s. The operator concluded optimal stent deployment when there were full apposition, adequate acute gain and the absence of edge tears. If underexpansion, malapposition or edge tear was noted on IVUS images, further balloon inflations were performed with the use of either higher pressure, larger balloon, or an additional stent. After further intervention, IVUS imaging was repeated to confirm optimal stent deployment.
Statistical analysis
All data are expressed as mean value±SD or as number (percentages). The baseline characteristics of the groups and follow-up data were compared by the t-test for continuous variables and by the χ2 statistic for noncontinuous variables. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) 12.0 (SPSS Inc., Chicago, IL, USA), and a p<0.05 was considered statistically significant.
Results
Patient and lesion characteristics
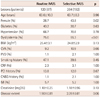
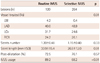
The study population consisted of 279 patients undergoing elective and emergency intracoronary implantation of TAXUS stent. Of these patients, 87 patients (120 lesions) underwent PCI under routine IVUS-guidance, whereas 192 patients (264 lesions) under selective IVUS-guidance. The two groups were well balanced in terms of baseline clinical characteristics, except that female patients were more common and dyslipidemia was less common in the selectively IVUS-guided group, which is presented in Table 1. The angiographic and procedural data are shown in Table 2. The proportion of the left anterior descending artery was higher in the selectively IVUS-guided group, and the proportion of the left circumflex artery was higher in the routinely IVUS-guided group. Implanted stent number per lesion was well balanced between both groups. The number of stents per lesion was 1.2 in the routinely IVUS-guided group and 1.15 in the selectively IVUS-guided group (p=0.33). However, stent length was longer in the routinely IVUS-guided group. Interestingly, both groups underwent post-balloon dilatation at comparable frequencies (72.5% vs. 76.1%, p=0.57). Even in patients under the routine strategy, the rate of IVUS imaging was not 100% but about 90%, which is still significantly higher than the rate in those under the selective strategy (89.2% vs. 68.2%, p<0.01).
Angiographic outcomes
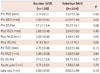
There was no difference in baseline reference vessel diameter and percent diameter stenosis (2.71 mm vs. 2.67 mm, p=0.50; 67.2% vs. 70.2%, p=0.06, respectively) (Table 3). However, minimal lumen diameter was slightly wider in the routinely IVUS-guided group (0.88 mm vs. 0.79 mm, p=0.05). In the case of the selectively IVUS-guided group, there were no differences in baseline reference vessel diameter and percent diameter stenosis between lesions with IVUS and lesions without IVUS (2.69 mm vs. 2.61 mm, p=0.28; 69.1% vs. 72.1%, p=0.12, respectively). After stent implantation, minimal lumen diameter was wider in the routinely IVUS-guided group (2.58 mm vs. 2.48 mm, p=0.03). In addition, percent diameter stenosis was smaller in the routinely IVUS-guided group (9.8% vs. 12.1%, p=0.05). Nonetheless, reference vessel diameter and acute gain did not show any difference (2.88 mm vs. 2.84 mm, p=0.45; 1.71 mm vs. 1.69 mm, p=0.75, respectively). Of the 384 lesions which received stent implantation, follow-up angiography was performed in 345 (89.8%). Of these, 336 (87.5%) angiograms were determined to be technically sufficient for analysis. At 6 to 9 angiographic follow-up, there were no statistically significant differences between the routinely IVUS-guided and selectively IVUS-guided groups with respect to reference vessel diameter (2.70 mm vs. 2.62 mm, p=0.12), minimal lumen diameter (1.98 mm vs. 1.98 mm, p=0.94), and percent diameter stenosis (27.0% vs. 24.7%, p=0.27). In terms of late loss, as with other parameters, no difference was found (0.59 mm vs. 0.50 mm, p=0.10).
Clinical outcomes
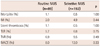
One-year clinical outcomes are presented in Table 4. Mortality rates were around 1% in both groups with no significant difference between them. In addition, the rate of MI was not statistically different between the two groups, which were both less than 5% (2.0% vs. 4.9%, p=0.44). In terms of stent thrombosis, no difference was found in the two groups. Accordingly, the rate of hard end points was not different. Soft end points, such as, TLR and TVR, showed no differences between the two groups (TLR; 5.7% vs. 6.8%; p=0.75, TVR; 6.9% vs. 9.5%; p=0.49). Taken together, the overall MACE (mortality, MI, stent thrombosis, TLR and TVR) during the 1 year follow-up period was not different between the two groups.
Discussion
The main finding of this study is that there were no significant differences in angiographic and clinical outcomes between the routinely IVUS-guided PCI and selectively IVUS-guided PCI groups.
Previous studies comparing angiography- vs. intravascular ultrasound-guided percutaneous coronary intervention
There have been some studies on the utility of routine IVUS during PCI in the pre-DES era. The results in the pre-DES era were different among the studies. In the OPTICUS study by Mudra et al.,15) a case-control study, they could not support the routine use of ultrasound guidance during PCI, and the results demonstrated that angiography-guided PCI could be performed with comparable clinical outcomes. Likewise, the AVID trial performed as a randomized controlled study failed to show reduction of clinical events for the entire subjects.17) Also, the PRESTO trial failed to demonstrate improved clinical outcomes, although IVUS influenced procedure characteristics.18) On the contrary, the CRUISE study, a multicenter study, demonstrated that TVR at 9 month-follow-up occurred significantly less frequently in the IVUS-guided group.12) Moreover, the TULIP study, which investigated long lesions, showed superior result in the IVUS group over the angiography group in terms of TLR and MACE.13) Choi et al.19) also reported that the use of IVUS guidance during stent implantation was associated with a significant decrease in 6-month TVR without increasing the procedure time, fluoroscopy exposure, contrast volume, or device utilization.19)
In the DES era, Roy et al.16) performed a study on the utility of IVUS during PCI with DES. In their study, IVUS was proven to give rise to less definite stent thrombosis and showed the tendency of less TLR. Therefore the study is thought to raise the possibility that routine IVUS use in the DES era could result in better clinical outcomes compared with angiography-guided PCI. However, this study was not intended to investigate the utility of routine IVUS vs. selective IVUS use in the DES era.
Comparison of two different strategies of intravascular ultrasound-guidance, routine vs. selective
In the present study, we compared two different strategies of IVUS-guidance, routinely vs. selectively IVUS-guided PCI rather than IVUS- vs. angiography-guided PCI, because IVUS-guidance is theoretically more helpful compared to angiographic guidance by assuring good apposition and optimal expansion which are both important factors to determine stent thrombosis or restenosis.
It is certain that IVUS is a useful tool to visualize vessel cross sections, thereby enabling us to confirm underexpansion, malapposition or edge tears. After confirming these unfavorable phenomena, we could perform additional interventions such as post-dilatation or stenting. Ultimately, these processes can improve long term clinical results. In fact, there was less definite stent thrombosis in the IVUS group in the study of Roy et al.16) although the cases were rare. The authors suggested that reduced minimal stent area and stent expansion along with greater residual disease are associated with stent thrombosis after DES implantation. IVUS use may allow the identification of these unfavorable factors and lead to appropriate subsequent treatment.
The remaining question is: which is the optimal strategy for IVUS-guidance, the routine use vs. the selective use? Our results showed that the selective use of IVUS was able to provide as good angiographic and clinical results as the routine use of IVUS during PCI. Therefore, considering our results, an experienced operator's ability to selectively use IVUS may save unnecessary use of IVUS during PCI. The results collectively suggest that adequate, but not absolute, IVUS use can produce good outcomes.
Angiographic outcomes after intravascular ultrasound-guidance
As with clinical outcomes, there have been contradicting studies in the BMS era. The OPTICUS study showed that repeat angiography revealed no significant differences between the IVUS-guided group and angiography-guided group with respect to dichotomous restenosis rate, minimal lumen diameter, and percent diameter stenosis.15) On the contrary, the CRUISE study demonstrated that the IVUS-guided group had a larger minimal lumen diameter by quantitative coronary angiography (QCA) and a larger minimal stent area at 9-month follow-up angiography.12) In addition, the TULIP study reported that at 6 months, MLD in the IVUS group was larger than that in the angiography group.13)
To our knowledge, there has been no report regarding angiographic results judged by QCA in the DES era. Moreover, there have been no studies comparing the two different strategies of IVUS-guidance. In our study, the angiographic data from the 'selective' IVUS-guidance group were comparable to those from the 'routine' IVUS-guidance group. Theoretically, IVUS is believed to produce more favorable angiographic results at follow-up angiography, because it gives us more chances to correct malapposition and underexpansion. However, considering our results, the use of IVUS in need is sufficient to produce results that are comparable to those of absolute IVUS use in the DES era. This might mean that an experienced operator could discriminate the case that is in need of IVUS and perform appropriate additional procedures and produce good results without routine IVUS use. In addition, the potential of DES to reduce the rate of restenosis may contribute to this favorable result of selection IVUS-guidance group.
Frequent use of post-dilatation may lessen the necessity of routine intravascular ultrasound-guidance during percutaneous coronary intervention
Coronary intervention is a sophisticated procedure. It has been well established that malapposition and underexpansion is associated with restenosis.20-22) As we know, post-dilatation is a very useful procedure after examination of IVUS to correct malapposition and underexpansion. According to the study of Roy et al., the rates of post-dilatation were 31.0% and 17.7% in the IVUS group and No IVUS group, respectively. Comparing with this result, a post-dilatation rate of about 75% is considered high in the present study. This high post-dilatation rate might have contributed to the comparable outcomes in the selectively IVUS-guided group, diminishing the beneficial effect which may be due to routine IVUS use. Furthermore, this raises a new hypothesis that the routine use of post-dilatation for optimized stent expansion would suffice for good outcome of coronary intervention instead of the routine use of IVUS.
Clinical implication
Most previous case-control studies and randomized clinical trials have dealt with both extreme ends, angiography- vs. IVUS-guidance PCI. However, recently, coronary interventionists all agree with the usefulness of IVUS. Thus, many physicians may be pressured to do routine IVUS-guidance. However, in the real world practice, most interventionists probably do not use IVUS in all patients. Instead, they may use IVUS at their discretion, if it is available in their catheterization laboratory. In such situations, our results may provide a helpful message. Given the relatively high percentage of post-dilatation, selective IVUS use would result in adequate clinical and angiographic outcomes. Therefore, when faced with suspicion for underexpansion and malapposition, we can perform post-dilatation without the routine use of IVUS. Furthermore, it is requested to perform a randomized study to determine whether routine post-dilatation is sufficient to obtain good results without IVUS.
Study limitations
Our study has several limitations. First, this study was a nonrandomized retrospective analysis from one center. Therefore, the results and conclusions are subject to the limitations inherent in this type of studies. Second, we collected patients with available QCA data. Therefore, patients who were excluded from the study by this reason could not be analyzed, resulting in the potential introduction of selection bias. Third, the baseline characteristics including gender, dyslipidemia, and vessel territory were different. These may have introduced bias in the analysis. Fourth, for the strategy of selective IVUS, there may be a wide spectrum of IVUS usage percent for different operators, because judgement for underexpansion, malapposition or edge tear is subjective.
 XML Download
XML Download