

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stress is a physical and psychological response to the perceived demands and pressures.1) Converging evidence from experimental and epidemiological studies indicates that there is an association between chronic psychological distress and cardiovascular disease.2) Psychological stress can cause endothelial distress and dysfunction in humans3)4) and animals.5)6) Enhanced sympathetic nerve activity (SNA) plays a major role in the development of atherosclerosis and endothelial dysfunction. Chronic physical pain and mental stress may enhance SNA, and alter the function of the sympathetic nervous system (SNS). Disequilibrium of the autonomic nervous system increases SNS activity at rest, along with a deficiency of SNS-mediated responses to certain stimuli, such as postural change or exercise.7) The link between psychosocial factors, such as stress and coronary artery disease, has drawn significant attention. Chronic stressful stimuli (such as work stress, marital stress, caregiver strain, low social support, and low socioeconomic status) have been linked to an increased risk of coronary artery disease and other adverse cardiac events.8) There is also evidence that emotional stressors can act as triggers for acute cardiovascular events.9) Moreover, the cultural construction of Hwabyung, a Korean culture-bound syndrome, is the occurrence of bodily symptoms in response to distressed emotions associated with the Korean way of perceiving and to intolerable and tragic life situations. Hwabyung usually occurs in middle-aged or older women and provides a way of conceptualizing and resolving emotional distress through somatic symptoms, such as chest tightness and palpitation among Korean elderly women.10)11)
Therefore, the present study tested the hypothesis that chronic emotional stress may exert negative effects on the myocardial function by measurement of the left ventricular (LV) strain and endothelial functions by measurement of flow-mediated dilatation (FMD) of the brachial artery.12)
Subjects and Methods
Study design and subjects
Consecutive postmenopausal female subjects with atypical chest pain, who complained of self-labeled chronic stress from December 2011 to July 2012, were enrolled in this study. Chronic stress was defined as suffering from stress for long periods, causing a person to be unable to relax.13) Participants were asked to complete the Symptom Checklist 90 Revised (SCL-90-R) survey, a cardiac echocardiogram, and an exercise stress test. Subjects with ischemic heart disease confirmed by coronary angiography and clinically significant arrhythmia were excluded. Patients with acute stress disorder defined as an anxiety disorder, characterized by a cluster of dissociative and anxiety symptoms occurring within one month of a traumatic event were also excluded. Other exclusion criteria were positive exercise stress tests, congestive heart failure, and significant valvular heart disease. The institutional review board approved this study, and all patients provided written informed consent before participation.
Echocardiographic evaluation
Standard 2D and strain echocardiographic examinations were performed on all subjects using a 3.5-MHz transducer on the Vivid 7 Dimension ultrasound equipment as they lay in the left lateral decubitus position (General Electric, Horten, Norway). Two-dimensional grayscale imaging (frame rate ≥70 seconds) and color Doppler tissue imaging (frame rate ≥115 seconds) were performed in the apical 2-chamber, 3-chamber and 4-chamber views, using a narrow sector angle. Images from the apical chamber views of the LV were obtained at the end-expiratory apnea and were stored in cineloop format for subsequent offline analysis. Three heartbeats were collected from each view, and a single selected cycle was analyzed off-line using an EchoPAC Dimension system (General Electric, Horten, Norway). Peak systolic strains were measured and averaged in order to assess the global longitudinal myocardial regional function (GLS). The endocardial borders were traced at the end-systolic frame, and an automated tracking algorithm outlined the myocardium in successive frames throughout the cardiac cycle. The tracking quality of each segment was verified (with subsequent manual adjustment of the region of interest if necessary), and myocardial motion was analyzed by speckle tracking within the region of interest bound by endocardial and epicardial borders. Inadequate tracked segments were automatically excluded from analysis. In this situation, local strain was calculated in each segment. GLS was obtained by averaging all segment strain values from the apical 4-chamber, 2-chamber, and long axis views.
Brachial artery measurements
Flow-mediated dilatation was performed using two-dimensional ultrasonography (Vivid 7, General Electronics Corp., Horten, Norway), using a modification of the method of Corretti et al.14) Measurements were performed on the subject's left arm after 10 to 20 minutes of rest in the supine position. The brachial artery was scanned longitudinally just above the antecubital crease using a 10-MHz probe. The diameter of the brachial artery was measured at the R wave of the surface electrocardiogram and at the interface between the tunica media and tunica adventitia of the anterior and posterior wall. Hyperemia was induced by inflation of a pneumatic cuff to 180 to 200 mm Hg (50 mm Hg higher than systolic blood pressure) for four minutes, on the most proximal part of the upper arm. The maximal diameter of the brachial artery was measured 45-60 seconds after the sudden deflation of the cuff. The percent brachial artery FMD induced by reactive hyperemia was expressed as the relative change from the baseline [percent FMD=100×{(diameter after hyperemia-baseline diameter)/baseline diameter}]. After 15 minutes, a third brachial artery scan was recorded at tre resting state, and the subject was administered a sublingual nitroglycerin 0.4 mg tablet if systolic blood pressure was ≥110 mm Hg. Relative changes in the brachial artery diameter from the baseline to the third examination were expressed as endothelium-independent vasodilatation with or without nitroglycerin. We measured each diameter three times during two heartbeats, and the mean values were used for the final analysis. An independent examiner, who remained blinded to the study, performed the measurements.
Stress assessment by questionnaires
The SCL-90-R is currently the most reliable and wide-ranging test for screening global psychological distress.15) The SCL-90-R is a validated 90-item multidimensional self-rating questionnaire originally developed to assess the psychopathology of psychiatric and medical outpatients. It has been extended to measure psychological distress in a wide range of populations.15)16) It assesses a broad range of physical and psychological symptoms that a subject might have experienced in the past seven days. Each of the 90 items is rated on a 5-point scale (ranging from 0 to 4), with higher values indicating greater impairment. The items build nine sub-scales: somatization, compulsivity, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The global severity index (GSI) is derived from all the items, and indicates the degree of overall psychological distress/impairment. Raw scores for the sub-scales and the GSI are between 0-4 (0=no distress to 4=maximal distress). These can be transformed into age and gender-specific normative values (T-value, normal range 50±10, higher values indicating greater psychological distress) by using a standardization reference table, and a total GSI T-score ≥50 is recommended as optimal for identifying patients with significant psychological distress.15)16)
Several recent studies have used the SCL-90-R as a measure of mental status and mental health issues in a non-psychiatric setting.17-19) The sub-scales show satisfactory reliability in patients with chronic pain. Cronbach's alpha ranges from α=0.71 to α=0.89, and the GSI is very consistent, with a Cronbach's alpha of α=0.97.20) The study participants were divided into two groups, based on whether their GSI was ≥50 (group A) or <50 (group B).
Statistical analysis
All data are expressed as the mean±standard deviation. Data were analyzed using standard statistical software (Statistical Package for the Social Sciences package version 11.0, Chicago, IL, USA), and comparisons of all measurements were made using the independent t-test for continuous variables of two groups and the Pearson correlation test for correlation. To evaluate if the myocardial longitudinal deformation is affected by chronic emotional stress, multivariate linear regression analysis was performed with adjustment of traditional cardiovascular risk factors. A p<0.05 was considered statistically significant.
Results
General characteristics of patients
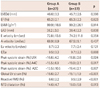
There were no significant differences between the high stress group (group A, GSI ≥50) and the low stress group (group B, GSI <50) in clinical, demographic, or laboratory variables (Table 1). The values of somatization, compulsivity, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism were significantly higher for group A (Table 1).
Strain echocardiographic findings
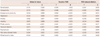
Global LV systolic function, LV chamber dimension, and LV mass index were normal in all patients with stress. There were no significant differences in the mitral inflow parameters or diastolic function between groups A and B. However, the values of the peak systolic LV strains of group A were significantly lower in three apical views, including the apical long axis view, the apical 4-chamber view, and the apical 2-chamber view, compared to group B (Fig. 1, Table 2). The GLS of group A was also significantly different compared with that of group B (-16.6±2.7% vs. -19.1±1.9%, p<0.001). Inter-observer and intra-observer variability was corrected for by independent analysis by two independent observers (C.K.I and H.S.K.) and by repeated measurement of these segments on another occasion by the same observer. The intra-observer regression coefficient was 0.92 and the inter-observer regression coefficient was 0.88. The main cause of inter-observer variability was the different locations of the sample volume. Once the sample volume was placed at a mutually agreed-upon location within the myocardium, measurements became virtually identical.
Brachial artery flow-mediated dilatation
The parameters of the endothelial function of patients are shown in Table 3. There were significant differences in the value of reactive FMD (6.6±2.2% vs. 9.5±2.9%, p<0.001) between groups A and B, and the same differences were observed with nitroglycerine (NTG)-induced dilatation (14.6±4.7% vs. 18.0±5.8%, p=0.013). The intra-observer and inter-observer variability for repeated measurements were 0.02±0.06 mm and 0.03±0.15 mm, respectively. The intra-observer regression coefficient was 0.87 and the inter-observer regression coefficient was 0.85 for echocardiographic measurements.
Correlation between the parameters of stress and myocardial or endothelial function
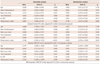
Global severity index showed significant correlations with GLS (r=0.384, p=0.002). The value of GLS correlated robustly with the nine items of the SCL-90-R, with the significant correlations being with paranoid ideation (r=0.472, p<0.001), phobic anxiety (r=0.405, p<0.001), anxiety (r=0.402, p=0.001), compulsivity (r=0.376, p=0.002), depression (r=0.330, p=0.008), and interpersonal sensitivity (r=0.329, p=0.008). Somatization, hostility, and psychoticism showed poor correlation with GLS (Table 3). GSI also showed significant correlations with reactive FMD (r=-0.583, p<0.001) and NTG-induced FMD (r=-0.342, p=0.006) (Fig. 2). Multivariate linear regression analysis showed that GSI was the only significant attributor to GLS (β=0.149, p=0.008) and reactive FMD (β=-0.200, p=0.041). However, age was the only significant attributor to NTG-induced FMD (Table 4).
Discussion
In this study, we demonstrated for the first time that myocardial longitudinal deformation and endothelial function is reduced in patients with chronic emotional stress, as assessed by the two-dimensional strain echocardiography and FMD. In addition, decreases in LV function and endothelial function were independently related to the severity of stress intensity as determined by the validated questionnaire, SCL-90-R.
There were no differences between the groups in conventional two-dimensional echocardiographic parameters, including ejection fraction, fractional shortening, relative LV wall thickness, LV mass index, and diastolic function, according to the severity of stress. However, global and segmental longitudinal LV strains were significantly reduced in the higher stress group. The longitudinal peak systolic strain/strain rate has been shown to be linearly correlated with the maximal value of the first LV filling pressure time derivative and with the peak elastance, which are both global measures of LV systolic function and contractility. Two-dimensional strain, as determined by speckle tracking, has recently been used for the quantitative evaluation of LV function. This method has been validated for the evaluation of longitudinal LV function.21) Subclinical LV dysfunction relates to the structure-function relationship and characterizes a preclinical stage of myocardial damage. This damage can be detected by a decrease in longitudinal myocardial function and the vulnerability of subendocardial fibers, which occurs before the development of abnormalities in conventional measures of LV performance.22)
Several mechanisms of myocardial damage concomitant with or downstream to the SNS activation have been proposed. Recent data suggest that elevated systemic levels of catecholamines are central to the pathophysiology of this disorder.23) However, the exact mechanism of catecholamine-induced myocardial damage is thought to be multifactorial. The postulated mechanisms include persistent activation of calcium channels, membrane damage, and microvascular spasm.24) Microvascular endothelial dysfunction can sensitize coronary circulation to the vasoconstrictor effects of catecholamines.25) Microvascular spasm and cardiac syndrome X are disorders predominantly associated with women, and particularly, postmenopausal women.26) Similar gender differences can be seen in transient LV dysfunction. In peripheral circulation, microvascular abnormalities are exacerbated by sympathetic nerve activation.27)
Chronic stress might be associated with impaired endothelial function. A variety of stimuli acutely influence FMD: a single high-fat meal and postprandial lipemia, mental stress,3) and probably by catecholamines, circulating levels of estrogen and progesterone,28) smoking, acute changes in glucose, and changes in sodium and calcium. In the present study, we compared FMD in high and low stress groups and evaluated the factors affecting endothelial function in patients with stress. Patients with higher stress exhibited decreased endothelial-dependent vasodilatation and endothelial-independent vasodilatation, and these parameters paralleled the severity of stress. Endothelial dysfunction is reflected by an impaired FMD response, which is determined from the forearm and coronary circulation. A vasodilatory stimulus is applied to the downstream vascular bed, eliciting flow-dependent dilatation of the upstream conduit vessel. As a control, the response of the brachial artery to sublingual nitroglycerine dilatation is recorded. The duration and the amplitude of brachial artery dilatation in response to NTG are more pronounced than during FMD. Our result showed that the severity of stress was the only significant attributor to reactive FMD, but not to NTG-induced FMD. With an increasing number of cardiovascular risk factors, smooth muscle dysfunction becomes apparent; thus, NTG response is progressively impaired independently from endothelial dysfunction.29)
Considering the strong correlation between stress parameters and LV strain/FMD, further clinical evaluation of myocardial and endothelial function with long-term follow-up is necessary, especially for patients with high initial stress levels. Given the association of physical or emotional stresses in patients with transient LV dysfunction, chronic stress may play a role in the change of LV function.
There are some limitations to this study. The number of patients in this study was relatively small, and the real duration of stress experienced by study subjects was not known.
Secondary, although we tried to exclude patients with ischemic heart disease according to the normal coronary angiography or negative Treadmill test, all subjects were not confirmed by coronary angiography; therefore, we cannot completely exclude the presence of significant coronary artery disease. As well-known, women tend to be false-negative in exercise stress test especially in patients without left anterior descending artery stenosis. Moreover, we did not check the coronary flow reserve or adenosine-stress MRI to exclude microvascular angina, which is a very common cause of atypical chest pain in postmenopausal women. However, microvascular angina have been found to present high levels of neuritucusm, i.e., anxiety, depression and somatic concerns, and our result may add the possible mechanism of atypical chest pain in microvascular angina. Although we assessed the severity of stress by questionnaire, a more objective assessment, such as functional magnetic resonance imaging or MIBG scanning is needed. In addition, the reversibility of LV functional impairment and endothelial dysfunction after stress treatment should be clarified through larger randomized studies.
In conclusion, chronic emotional stress may exert negative effects on LV and endothelial function, which might be associated with the severity of stress. This study provides a possible mechanism by which stress may be associated with an increased risk of cardiovascular dysfunction. However, longitudinal studies employing a large population are required to determine the pathophysiology and prognostic implications of endothelial dysfunction in patients with chronic stress.



 XML Download
XML Download