

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Peripheral artery disease (PAD) is a significant medical problem, particularly among the elderly population1-3) because it is associated with a significantly elevated risk of cardiovascular disease morbidity and mortality.2)
Elderly patients who undergo surgical intervention have higher post operative mortality.4)5) Hence, percutaneous transluminal angioplasty (PTA) has become an accepted alternative to bypass surgery in patients with PAD.1)
However, determining the appropriate access strategy for peripheral vascular interventions often requires a much greater degree of planning and foresight than with cardiac catheterization.
Occasionally, PTA through a bypass graft is required to improve inflow or run-off vessels as well as to treat graft stenosis or occlusions as an alternative treatment option to reoperation in patients at high surgical risk.
We report a case in which we successfully performed PTA of contralateral inflow iliac artery and superficial femoral artery via femorofemoral bypass graft in a PAD patient.
Case
A 73-year-old male with a long-standing left common iliac artery occlusion underwent femorofemoral crossover grafting 4 years ago. In addition, he had angioplasty and stenting of the right superficial femoral artery on different occasions within the previous year at other hospitals. The patient reported mild improvement in claudication symptoms for a few months only after each of these procedures.
He came to our hospital with a disabling bilateral lower extremity claudication. He had a past medical history of hypertension and diabetes in addition to a 60 pack-year history of smoking. For the past two months, the patient complained of claudication in both lower legs as well as severe pain in the right lower leg at rest (Rutherford category 4). On physical examination, he had a faintly palpable dorsalis pedis pulse in the right foot. Ankle brachial indices indicated a score of 0.34 on the right and 0.60 on the left. Computerized tomography angiography revealed a patent graft, but it also showed a high-grade focal stenosis of the right common iliac artery and a total occlusion of the superficial femoral artery (Fig. 1). Due to patient's refusal to undergo surgical revascularization, endovascular treatment was planned for the extensive iliofemoral occlusive disease.
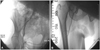
Arterial access was obtained in the left common femoral artery below the level of femorofemoral crossover graft. Angiography showed that the right common iliac artery had severe stenosis of a focal 80% lesion (Fig. 2A), and the right superficial femoral artery had total occlusion (Fig. 2B). Right external and internal iliac, common femoral and profunda femoris arteries were patent. Femorofemoral crossover graft was also patent.
A 5 Fr glide catheter (Terumo, Tokyo, Japan) and a 0.035 inch radiofocus angled soft guide 263 cm wire (Terumo, Tokyo, Japan) crossed the stenosis of the right common iliac artery via femorofemoral crossover graft. Then, the stenosis was predilated using a 7.0×80.0 mm balloon catheter (PowerFlex; Cordis, Miami, FL, USA) at 10 atm for 120 seconds. In addition, 8.0×100 mm self expandable stent (Smart, Cordis, Miami, FL, USA) was deployed in the right common iliac artery. After stent placement, control angiogram showed no significant residual stenosis or dissection (Fig. 3). Using a 0.035 inch straight Terumo wire with a backup catheter (5 Fr multipurpose catheter; Cordis, Miami, FL, USA), successful wiring of the superficial femoral artery was performed by intraluminal wire passage without significant dissection. Total occlusion was dilated using a 5.0×80.0 mm balloon catheter (PowerFlex; Cordis, Miami, FL, USA) at 10 atm for 120 seconds and 7.0×80 mm balloon catheter (PowerFlex; Cordis, Miami, FL, USA) at 6 atm for 120 seconds. This resulted in no significant residual stenosis or dissection through the superficial femoral artery (Fig. 4).
After a successful angioplasty, the patient had no residual symptoms (Rutherford category 0); the right ankle-brachial index improved from 0.34 to 0.83 and the left ankle-brachial index improved from 0.60 to 0.88.
Discussion
Percutaneous transluminal angioplasty is an alternative revascularization technique for PAD. Because stenting is less invasive compared to endarterectomy or bypass graft, advanced-age patients or patients at high surgical risk are more likely to be candidates for PTA.
Arterial access problems frequently complicate percutaneous interventions in PAD of the lower limbs. Typically, interventions at the iliac artery level are performed either in a retrograde approach after puncture of the ipsilateral femoral artery or in a crossover technique by obtaining arterial access on the contralateral side of the lesion, and subsequently maneuvering the guide wire across the aortic bifurcation into the diseased vessel. These procedures are often difficult and fraught with potential local complications. The choice of approach varies between institutions and for individual patients. Due to the fact that the number of patients who have undergone reconstructive vascular surgery is continuously increasing, we are faced with an increasing demand for peripheral artery revascularization in patients with bypass graft. For those patients, the traditional approach has been employed through a transradial approach or the brachial artery in order to avoid direct puncture of the graft site due to possible postprocedural complications.6)7) However, this approach requires special effort in the optimization of the backup and the stabilization of the guiding catheter. This procedure often requires a good strategy, appropriate catheter manipulations and the use of specific technical maneuvers. Moreover, nerve injury or postoperative radial artery occlusion remains a major concern. Sometimes, given its distance from the radial artery and the brachial artery, the femoral artery stenosis may not be reached using this approach.
We would like to recommend the convenience of the procedure over PTA via graft vessel. Because larger devices are required for iliac artery and femoral artery stenosis compared to coronary intervention, it is convenient to use the backup and the stabilization of the guiding catheter, and also easy to manipulate the use of specific technical maneuvers, such as wire and catheter.
In this case, it was possible to salvage a successful outcome that would only have been possible with PTA of contralateral inflow iliac artery and superficial femoral artery via femorofemoral bypass graft in a patient of PAD.



 XML Download
XML Download