

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In the last 3 decades of medical development, transcatheter treatment of coarctation of aorta with balloon angioplasty and stent implantation has now become an acceptable alternative to surgical repair. However these procedures may result in complications, such as intimal tearing, neo-intimal hyperplasia, restenosis of the lesion, aneurysm formation, dissections, and, rarely, even fatal aortic rupture.1-3) When the usual balloon expandable stents are used, some degree of vascular wall injury may be inevitable during the forced immediate dilatation of the stenotic lesion. However, a nitinol self-expandable stent, when deployed at the coarctation site, produces low constant radial force, which may result in a gradual widening (stretching) of the stenotic lesion, instead of tearing vascular wall structures ('stretching rather than tearing'), leaving less tissue injury.4)5) And when the result of the self-expansion of the stent is not enough, further in-stent balloon dilatation can be done easily immediately or after an appropriate interval. We report our experience with a nitinol self-expandable stent for the treatment of native aortic coarctation in an adolescent patient.
Case
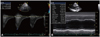
An 18-year-old female, height of 165 cm and body weight of 55 kg, was diagnosed with a native aortic coarctation. She has no significant difficulty in her usual activities and exercises. She has complained only of intermittent headache. Her blood pressure (BP) measurements were 123/64 mm Hg and 123/62 mm Hg at her right and left arm, while 86/47 mm Hg and 83/49 mm Hg at her right and left ankle, showing 50 mm Hg higher BP in the upper extremities (Table 1). On echocardiographic study, discrete aortic coarctation was diagnosed with the peak pressure gradient across the stenotic lesion of 50 mm Hg by Doppler study (Fig. 1). On chest CT angiogram a discrete narrowing at the isthmic portion of the aortic arch due to a posterior shelf lesion was seen (Fig. 2). The narrowest dimension of the stenotic lesion was 4-5 mm, and the dimensions of the pre- and post-coarctation descending aorta were 16 mm and 19 mm, respectively (Fig. 2). The distance from the origin of left subclavian artery to the coarctation site was 24 mm.
A 20 mm self-expandable nitinol stent (Hercules vascular stent 20×60 mm, S&G Biotech, Seongnam, Korea) was deployed across the coarctation site, without previous balloon dilatation procedure (Fig. 2). No further balloon dilatation was done immediately after the stent deployment to avoid unnecessary tissue injury. Immediately after the procedure, the peak pressure gradient across the coarctation site decreased from 50 mm Hg to 20 mm Hg (Table 2), and the dimension of the stenotic lesion shown by the stent waist somewhat increased from 4-5 mm to 8 mm on angiography and plain chest X-ray images (Fig. 2). We decided to wait and see for further self-expansion of the stent.
Three months after the procedure, the dimension of the stent waist had enlarged gradually up to 13 mm on plain X-ray and 11.5 mm on CT images (Fig. 3). Further interventional procedure, such as instent low-pressure balloon dilatation, was suggested to trim the remnant waist of the stent. But the patient and her parents were happy with the present status and refused any further procedures.
One year after the stent deployment, the dimension of the stent waist further increased slightly up to 14 mm (Fig. 4). The BP measurements in the upper extremities somewhat decreased, while the BP measurements in the lower extremities increased significantly up to higher than those of the upper extremities (Table 1). On echocardiographic study, the exact Doppler pressure gradient across the pervious stenotic site was not available because the images of the previous stenotic lesion were poor and definite flow turbulence was not found, suggesting the remnant stenosis not significant. Subjectively, as she felt no significant difficulty in her physical activity before the stent insertion, she felt not so much difference in her physical activity after the stent insertion. However, she said she felt more warmness in her lower extremities after the stent insertion than before, having more tolerance for cold weather when she was wearing skirts.
Discussion
A nitinol self-expandable stent exerts low constant radial force after the deployment in the stenotic lesion and results in gradual widening of the stenotic lesion. It is flexible and easy to deploy and can be used safely in patients with aortic coarctation, leaving less tissue injury. Because the radial force of the self-expandable stent is not so strong, self-expansion ability of the stent depends on the compliance of the stenotic lesion to the radial force. In the native virgin state of coarctation of aorta, where no intimal injury was made by the previous surgery or interventional procedures, the use of nitinol self-expandable stent can be desirable to avoid tearing injury on the vascular wall structure. In the restenosis lesions after the previous balloon dilatation or surgery where the compliance of the stenosis lesion to the radial force is not good, the self-expansion ability of the stent may not be enough. In these cases, further in-stent balloon dilatation or balloon expandable stent insertion can be considered.
In using a self-expandable stent in a native coarctation patient, we do not recommend any previous balloon dilatation prior to the stent insertion or any further balloon dilatation immediately after the stent insertion to avoid unnecessary tissue injury. If self expansion of the stent doesn't look sufficient after several months' observation period, in-stent low pressure balloon dilatation procedure can be easily done to relieve the remnant stenosis.
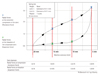
Mechanical properties of stress (external force inducing deformation of the stent) and strain (degree of deformation, change in the diameter of the stent) of the self-expandable stent showed a kind of linear relation pattern in a limited range of the stent dimension. As the loaded stress increases, the strain increases in linear relationship initially, but after the stress (external force) reaches a certain level, a much larger strain (deformation) is observed at a small change of the stress. And some different curves were observed at the time of stress loading and stress unloading (Fig. 5).4)5) The resistance force of the stent measured during the external concentric force (stress) was being loaded was larger than the expansion force of the stent measured during the external concentric force was being unloaded. While unloading the stress, as the diameter of the stent (strain) is recovered, the measured stress (radial force exerted by the stent) decreased rather steeply.
In an experiment of concentric compression and relaxation of the self-expandable nitinol stent (S&G Biotech, Seongnam, Korea), the radial forces of the stent were measured at varying diameters of the stent. The 20 mm diameter stent was tightened gradually by a ringed device to the diameter of 5 mm and, thereafter, loosened gradually to the diameter of 20 mm (Fig. 5). Generally, the smaller the diameter the stent was reduced to, the stronger the radial force exerted by the stent was observed. As the diameter of the stent recovered, the radial force exerted by the stent decreased steeply. When the diameter of the stent increased to a certain level, the radial force exerted by the stent (equivalent to the stress) became quite weak not enough to expand the stent further significantly.
When a self-expandable stent of 20 mm diameter was inserted into the 5 mm stenotic lesion in this case, the radial force produced by the stent might be enough to gradually widen the stent waist during the early period after the stent insertion. It might be reasonable to wait and observe the self-expansion of the stent over a several month period. As the diameter of the self-expandable stent increased over several months, the radial force exerted by the stent decreased steeply to an insignificantly low level, allowing no significant further self-dilatation of the stenotic lesion. At this point, instent balloon dilatation procedure can be helpful.
For the discrete stenotic lesion of the descending aorta in this case, the stent with a shorter length (40-45 mm) was sought first. However, for the diameter of 20 mm, only 60 mm length stent was available from the product company then. We decided the use of the 60mm length stent could be an acceptable option in the adult sized patient of this case.
In conclusion, for an 18-year female with native aortic coarctation, a self-expandable nitinol stent was used successfully. No balloon dilatation procedure was done before or immediately after the stent insertion. Over the following 3-month period, gradual self-expansion of the stent resulting in gradual widening (stretching) of the stenotic lesion to an acceptable dimension was observed. After 1 year, a little further widening of the stent waist was observed.
For some patients with native aortic coarctation, where the compliance of the stenotic lesion is well maintained, the use of a nitinol self-expandable stent can be the best treatment option to relieve the stenosis avoiding unnecessary vascular wall injury.





 XML Download
XML Download