

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Variant or Prinzmetal's angina, characterized by transient resting ST-segment elevation on electrocardiogram (ECG), was first described by Prinzmetal et al.1) in 1959. He emphasized the occurrence of resting angina and the observation of reversible ST-segment elevation during angina. Diagnosis of variant angina is of great importance, as treatments thereof are effective. However, spontaneous attacks are often difficult to document. Maseri et al. reported that coronary artery vasospasm occurred spontaneously during coronary angiography in only 17 of 107 variant angina patients.2) In 1949, Stein3) proposed that ergonovine may be clinically useful in the diagnosis of patients with suspected coronary artery vasospasm. Currently, ergonovine provocation test is a mainstay of clinical practice for diagnosing variant angina.
Here, the case report of a male patient who presented with atypical chest pain and underwent coronary angiography and ergonovine provocation test is described. Coronary angiography did not show any significant stenosis in coronary arteries and ergonovine provocation test was negative. The patient was prescribed a proton pump inhibitor and prokinetics for symptom control. After 5 years, he visited the emergency room (ER) with an acute myocardial infarction due to coronary artery vasospasm, drawing attention to the false negative results of the ergonovine provocation test.
Case
A 49-year-old-man visited our outpatient clinic on October 1, 2007 with atypical chest pain that had started 2 months before. He complained of crushing chest pain that lasted for 5 to 10 seconds. The pain usually occurred early in the morning and was not related to exercise. The pain would disappear without any specific treatment. ECG showed no definite ST-segment changes. Echocardiography also showed normal left ventricular systolic function and there were no regional wall motion abnormalities. He was not taking any medication except for a budesonide inhaler and mometasone (topical corticosteroid) for treatment of asthma.
The patient underwent coronary angiography and ergonovine provocation test. Ergonovine 0.2 mg was injected twice intravenously at a 5-minute interval. We achieved cineangiogram at 90 seconds after each ergonovine injection. Coronary angiography showed no significant lesions in the coronary arteries and the intravenous ergonovine provocation test was negative (Fig. 1). There was no chest pain, ST-segment changes, or coronary artery vasospasm noted during the ergonovine provocation test. We did not prescribe any antianginal medication such as nitroglycerine before the ergonovine provocation test, which would have affected the results of the test. Esophagogastroduodenoscopy showed hemorrhagic gastritis and erosive duodenitis. The gastrointestinal tract was thought to be the source of the pain and he was prescribed a proton pump inhibitor and prokinetics for pain relief.
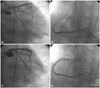
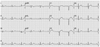
After 5 years, on January 15, 2012, he visited the ER with sudden onset of chest pain while sleeping. The characteristics of the chest pain were very similar to the pain that occurred in 2007. In the ER, the chest pain was relieved by sublingual nitroglycerin and he was admitted to the coronary care unit. After several hours, the chest pain recurred and the patient complained of dizziness, nausea, and vomiting. His blood pressure dropped to 76/41 mm Hg, and he had symptomatic sinus bradycardia. ECG showed no definite ST-segment changes (Fig. 2), but troponin I was elevated to 90.3 ng/mL. Suspicious of non ST-segment elevation myocardial infarction combined with cardiogenic shock, we performed coronary angiography. Coronary angiography showed no significant stenosis of the left main, left anterior descending, or left circumflex coronary arteries (Fig. 3), but total occlusion with distal Thrombolysis in Myocardial Infarction flow grade 2 in the distal right coronary artery, posterior descending artery, and posterolateral branch bifurcation segment was observed (Fig. 4). After intra-coronary nitroglycerin injection, the occluded segment was dilated (Fig. 5) and chest pain was slowly relieved. Blood pressure and heart rate were also stabilized. Echocardiography showed akinesia of the apical anterior, septal, and inferior walls. Chest pain did not recur after taking diltiazem and nicorandil. The patient is now under outpatient clinic follow up without any further event.
Discussion
The incidence of variant angina is 2-20% in Western populations4) and 4.4% in the Korean population.5) The incidence appears to have declined over the past few decades, which may be attributable to smoking cessation and more frequent use of calcium channel blockers.6) The mechanism of variant angina is coronary artery vasospasm with or without atherosclerotic coronary artery disease.7) Calcium channel blockers, which are extremely potent in preventing episodes of coronary vasomotor tone abnormalities, are especially effective in preventing episodes of myocardial ischemia in variant angina patients. β-adrenergic blocking agents and therapies directed against platelet aggregation are ineffective in preventing episodes of ischemia in these patients.8) Variant angina can lead to ventricular fibrillation and even sudden cardiac death. Thus, it is very important to diagnose variant angina correctly.
The key to diagnosing variant angina is to detect episodic ST-segment elevation often accompanied by chest pain, usually occurring at rest. However, as in our case as well as the studies by Feldman et al.,9) there are cases of variant angina without ST-segment changes. It is also difficult to document 'episodic' ST-segment elevation. Ergonovine maleate, an ergot alkaloid, is a direct acting smooth muscle constrictor. Heupler et al.10) reported that ergonovine may provoke attacks of variant angina. Ergonovine is thought to act directly on vascular smooth muscle to increase arterial and central venous pressure, and to decrease venous compliance. Intravenous injection of ergonovine is most commonly used to provoke coronary artery vasospasm.11)12) According to Waters et al.13) the sensitivity of intravenous ergonovine provocation test was 100% using anginal chest pain as the diagnostic criterion and 94% using ST-segment elevation.
After a negative ergonovine provocation test, our patient presented with acute myocardial infarction accompanied by cardiogenic shock and symptomatic bradycardia due to coronary artery vasospasm. It is possible that the patient had suffered from non-anginal chest pain 5 years ago and then developed coronary vasospasm 5 years later. However, the characteristics of chest pain in 2007 and 2012 were very similar in nature (crushing), location (substernum) and onset time (in the early morning), indicating that the two events shared a common etiology. The negative result on the ergonovine provocation test in our patient could be related to the sensitivity of the test. In 2004, Sueda et al.12) reported the incidence of coronary artery vasospasm after intracoronary ergonovine injection in 596 consecutive Japanese patients to be 2.2-2.6 times higher than previous reports of intravenous ergonovine provocation. The clinical impact of intracoronary ergonovine provocation test in diagnosing variant angina needs further study.
Ergonovine provocation test is the key to diagnosing variant angina. Our case exhorts that ergonovine provocation test is far from perfect, and one should always consider the possibility of false negative results, and intracoronary ergonovine provocation tests may be helpful where appropriate. Vasodilators such as calcium channel blockers or nitrates, as well as discontinuation of smoking and alcohol consumption should be considered in patients with a clinical manifestation suggestive of variant angina, even after a negative ergonovine provocation test.



 XML Download
XML Download