

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Variant angina pectoris (VAP) was first described by Prinzmetal et al.,1) and is a syndrome of ischemic pain accompanied by ST-segment elevation that occurs at rest and without exertion. Transient increases in coronary vasomotor tone or vasospasm are the pathogenic mechanism underlying Prinzmetal or VAP.2) Coronary artery spasm in VAP has been found to be associated with systemic alteration in nitric oxide (NO) production or an imbalance between endothelium-derived relaxing and contracting factors that results in complications, most often myocardial infarction, life-threatening arrhythmias, or sudden cardiac death.3-5)
Natriuretic peptides, comprising atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP) and C-type natriuretic peptide (CNP), are a family of polypeptide mediators that play an important role in the regulation of cardiovascular homeostasis by maintaining blood pressure and extracellular fluid volume.6-8) ANP and BNP are mediators that are mainly secreted by the myocardium in response to many pathophysiological conditions,6-8) while CNP is mainly produced by vascular endothelium and contributes to smooth muscle relaxation, where it may exert its autocrine/paracrine roles in vascular tone and muscle cell growth.6-8) The contribution of endothelial mediators to the effects of CNP on the coronary circulation is unclear and poorly characterized. Therefore, we investigated the value of CNP as a surrogate marker for detection of coronary artery spasm in VAP, and estimated a threshold value for this purpose.
Subjects and Methods
Patients
Between July 2005 and May 2008, a total of sixty-six patients (mean age: 51±11 years, M : F=40 : 26) who underwent coronary angiography on suspicion of angina and who were diagnosed with VAP by acetylcholine-induced spasm provocation test (SPT) were enrolled. Patients were divided into two groups: the SPT (-) group (n=23) and the SPT (+) group (n=43), members of which were diagnosed with VAP based on the definition of VAP applicable for acetylcholine-induced SPT, that is, focal occlusion greater than 70% of the luminal diameter with clinical symptoms or ST-segment change on electrocardiography (ECG).9)
This study was approved by the Ethics Committee of St. Mary's Hospital. Patients were informed of the investigative nature of the study and written informed consent was obtained before enrollment.
Coronary angiography
Coronary angiography was performed in all patients using a femoral approach with standard catheters placed in conventional positions. Nitroglycerin was not administered before angiography. For SPT of the coronary artery, intracoronary injection of acetylcholine was administered according to the method of Okumura et al.10) Incremental doses of 20 and 50 µg acetylcholine were injected into the right coronary artery, and 20, 50, and 100 µg doses were injected into the left coronary artery. ECG and coronary angiography were repeated to confirm the presence of coronary artery spasm. The angiograms were analyzed by two experienced angiographers.
Biochemical assays
Concurrently, blood samples for the analysis of plasma CNP and N-terminal pro-brain natriuretic peptide (NT pro-BNP) concentration were drawn into ethylenediaminetetraacetic acid-plasma vacuum containers. Plasma CNP (catalog No. E0721h) concentration was assayed with an immunoassay (USCNLife Science & Technology co., Ltd., Wuhan, China) in which there is no cross-reactivity with plasma NT pro-BNP. The detectable range for assay was CNP 0-500 pg/mL (sensitivity 3.9 pg/mL).
Statistical analysis
All analyses were performed using the SAS statistical software version 9.1 (SAS Institute Inc., Cary, NC, USA). For comparisons between the SPT (-) and (+) groups, mean±standard deviations and proportions were compared using the unpaired t-test and chi-square test, respectively. The relationships between multiple parameters and plasma CNP or NT pro-BNP concentration were assessed using Spearman's correlation coefficient by rank. After adjustment for age and gender, multivariate logistic regression analysis was performed for detection of the independent factors associated with VAP via acetylcholine-induced SPT. A receiver operating curve was used to determine the cut-off value for plasma CNP concentration as a predictor of the probability of the presence of VAP via acetylcholine-induced SPT. Statistical significance was considered at p of less than 0.05.
Results
Clinical characteristics
Among the sixty-six patients subjected to the intracoronary acetylcholine-induced SPT, 43 were SPT positive {SPT (+) group; mean age: 51±10 years, M : F=30 : 13} and 23 were SPT negative {SPT (-) group; mean age: 49±12 years, M : F=10 : 13} (Table 1).
Results for comparison according to acetylcholine-induced spasm provocation test
Basophil percentage and blood urea nitrogen concentration were significantly increased in the SPT (+) group relative to the SPT (-) group (basophil percentage, 0.6±0.5% vs. 0.4±0.2%, p=0.039; blood urea nitrogen, 15.8±4.9 mg/dL vs. 13.2±2.8 mg/dL, p=0.014, respectively) (Table 1).
Plasma CNP and creatine kinase myoglobin band (CK-MB) concentrations were significantly increased in the SPT (+) group relative to the SPT (-) group {CNP, 5.268±1.800 pg/mL vs. 3.342±1.150 pg/mL, p=0.002 (Fig. 1); CK-MB, 2.54±1.03 ng/dL vs. 1.86±0.96 ng/dL, p=0.019, respectively} while plasma high sensitivity C-reactive protein (hs-CRP) and NT pro-BNP concentrations were not significantly different between the SPT (-) group and SPT (+) groups (hs-CRP, 2.76±4.99 mg/L vs. 3.13±4.88 mg/L, p=0.789; NT pro-BNP, 49±47 pg/mL vs. 57±63 pg/mL, p=0.818, respectively) (Table 1).
Associations among biomarkers
Plasma NT pro-BNP concentration was positively correlated with that of CK-MB (r=0.543, p<0.0001) and negatively correlated with heart rate (r=-0.339, p=0.026, respectively) (Table 2). Plasma CNP concentration was negatively correlated with heart rate (r=-0.403, p=0.030) and total cholesterol level (r=-0.369, p=0.041, respectively) (Table 2).
Predictability of coronary artery spasm
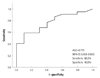
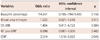
Plasma CNP concentration was independently associated with coronary artery spasm in patients with VAP via acetylcholine-induced SPT after adjustment for age and gender {odds ratio: 2.014 (95% confidence interval: 1.016-3.992), p=0.045} (Table 3). A CNP cut-off value of 4.096 pg/mL was found to have a sensitivity of 68.2% and a specificity of 40.0% for predicting the probability of VAP presence via SPT (Fig. 2).
Discussion
The natriuretic peptide system includes three known peptides: ANP, BNP, and CNP. Although ANP and BNP rise excessively in patients with cardiovascular diseases and are powerful neurohormonal indicators of left ventricular function and prognosis in congestive heart failure (CHF), the role of plasma CNP in human circulation has appeared to be minor and has been poorly characterized.6-8)
C-type natriuretic peptide, a new member of the natriuretic peptide family identified in both the animal and human brain, terminates in the second cysteine residue, thereby lacking a further C-terminal extension, and its level in humans is 10-fold higher than those of ANP and BNP.11)12)
Recently, some studies have reported the pathophysiological role of CNP as a predictor of endothelial vasomotor response in patients with CHF.13)14) Although it is well known that CNP is a peptide produced by the vascular endothelium with vasodilative properties,15-17) our study is the first to demonstrate the pathophysiological role of CNP in patients with VAP.
The most important finding in the present data was that plasma CNP concentration was higher in the SPT (+) rather than SPT (-) group. Until recently, most research has reported that CNP level was not only inversely related to a number of cardiovascular risk factors but also that CNP exhibited significant negative associations with pulse wave velocity for arterial stiffness and intima-media thickness for early atherosclerosis and positive association with flow mediated dilation for endothelial function.18-21) This has been well demonstrated by previous reports into the association with endothelial dysfunction in patients with VAP22) as well as those with microvascular angina.23-26)
However, our present result showed that plasma CNP concentration was higher in the SPT (+) group, which is known to be a type of endothelial dysfunction. Our investigators could carefully elicit a new understanding as follows. Coronary atherosclerosis is initiated by endothelial dysfunction due to inflammation and increased low density lipoprotein-cholesterol (LDL-C) levels, followed by the deposition of lipids and macrophages from the lumen into the inner layer of the coronary artery, resulting in plaque formation.27) In short, endothelial dysfunction is likely to be the earliest event in the process of atherosclerotic lesion formation. Therefore, plasma CNP concentrations in present study may have an impact on the regulation of endothelial function in accordance with atherosclerotic progression in patients with VAP. Further analysis is warranted to develop clinical applications of this concept.
Additionally, in terms of the vascular endothelium, Palmer et al.21) demonstrated that circulating CNP concentration was related to cardiac hemodynamic load and ischemic burden. In contrast, Naruko et al.19) suggested that a paracrine and autocrine system of CNP may be important in controlling the neointimal growth of vascular smooth muscle cells after percutaneous coronary intervention in humans. Moreover, in animal studies addressing the role of the cardiovascular NO system in the actions of CNP, Costa et al.20) demonstrated that CNP increased NO excretion, which would induce a reduction in cardiac myocyte contractility and relaxation of the vascular smooth muscle, thereby suggesting an association with endothelial function. Although our results are in agreement with previous reports, further research using a larger population is warranted.
Kuo et al.28) reported that the myocardium regularly produces or releases CNP in patients with symptomatic paroxysmal supraventricular tachycardia (PSVT) and normal left ventricular systolic function and brief periods of rapid atrial pacing, and that PSVT or electrophysiological studies did not change the production and/or release of CNP. Lupattelli et al.29) suggested that CNP was not altered in patients affected by hypercholesterolemia. Nevertheless, the levels of high density lipoprotein-cholesterol were closely related to those of CNP. In the present study, heart rate and total cholesterol level were significantly correlated with the CNP level and thus further analysis is warranted to address this discrepancy.
This study has some limitations. First, blood samples were not collected from the coronary sinus but from the femoral artery. Second, associations with various vasoactive agents, such as endothelin, angiotensin II, and serotonin, were not assessed. Lastly, there was a selection bias in this study's patients. To overcome this methodological limitation, more research in patients with significant coronary artery disease (>50% stenosis in ≥1 coronary artery) is warranted.
In conclusion, coronary atherosclerosis is initiated by endothelial dysfunction due to inflammation and increased LDL-C levels, which is followed by the deposition of lipids and macrophages from the lumen into the inner layer of the coronary artery, resulting in plaque formation. Therefore, increased plasma CNP concentration in patients with VAP may have an impact on the regulation of endothelial function in accordance with the progression of atherosclerosis. Further analysis is warranted to develop clinical applications of this finding.



 XML Download
XML Download