

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Calcifications are present almost solely in relation to atherosclerosis in the coronary vessels except for individuals with chronic kidney disease.1) Therefore, coronary artery calcium score (CACS) has been used as a useful surrogate marker for coronary atherosclerosis burden. Furthermore, CACS provides prognostic information in asymptomatic population.2-5) From these data, the use of CACS for risk stratification in asymptomatic population is advocated by professional guidelines.6-8)
Coronary computed tomographic angiography (CCTA) has been introduced as a noninvasive imaging modality to directly assess the degree of coronary artery stenosis.9)10) The outstanding diagnostic accuracy of CCTA has been demonstrated by prospective multicenter studies using coronary angiography (CA) as the reference standard.11)12) Widespread use of CCTA revealed a non-negligible prevalence of non-calcified plaque (NCP) in subjects with CACS of zero, who have very low probability of future cardiac adverse events.13-15) In symptomatic patients, NCPs are predictive of myocardial hypoperfusion and future coronary events.16-18) However, the clinical predictors and the prognosis of NCP in asymptomatic subjects with zero CACS have not been fully evaluated.19)
Therefore, we evaluated the association of standard risk factors with NCP, and the prognosis of NCP in middle aged asymptomatic subjects with CACS of zero using CCTA.
Subjects and Methods
Study population and design
Between December 2005 and January 2008, we enrolled 5632 consecutive subjects who underwent CCTA using 64-slice multi-detector row computed tomography (MDCT) at Seoul National University Bundang Hospital (SNUBH). We included asymptomatic individuals who had CCTA as part of general health evaluation in a health promotion center. We excluded subjects as follows: 1) insufficient medical records or inadequate imaging for analyses (n=24); 2) age less than 35 or more than 75 years (n=195); 3) subjects who had CACS >0 (n=922) for current analyses. As a result, 4491 middle-aged individuals with CACS of zero were finally enrolled. The study protocol was approved by the Institutional Review Board and all patients provided written informed consent.
Imaging data acquisition and analyses
Data acquisition and image post-processing for CCTA and CACS were done in accordance with the Society of Cardiovascular Computed Tomography guidelines,20) and detailed methods were described in previous manuscript.21)
Coronary artery calcium scores were measured using the scoring system previously suggested by Agatston et al.22) The CCTA was performed on a 64-slice MDCT scanner (Brilliance 64, Philips Medical Systems, Best, The Netherlands). Beta blockade with intravenous esmolol, 10 to 30 mg (Jeil Pharm. Co., Ltd., Seoul, Korea) was used to achieve a heart-rate of <70 beats/minute. Eighty milliliter of intravenous contrast (Iomeron 400, Bracco, Milan, Italy) at a rate of 5 mL/sec followed by 50 mL saline chaser were injected intravenously. A scanning protocol was as follows: 64×0.625 mm section collimation, 420-ms rotation time, 120-kV tube voltage, 800-mA tube current. All scans were performed with electrocardiogram-gated dose modulation. The mean radiation exposure of CCTA was 13.21±0.82 mSv (13.21± 0.83 for male and 13.33±0.79 for female).
Plaque assessment was independently performed by 2 experienced radiologists (Sang Il Choi, years of experience after board certification: 8 years; Eun Ju Jeon, years of experience after board certification: 6 years). Coronary atherosclerosis was defined as any tissue structures >1 mm2 that existed either within the coronary artery lumen or adjacent to the coronary artery lumen, which could be clearly discriminated from surrounding pericardial tissue or the vessel lumen itself. Each lesion was identified with a multiplanar reconstruction technique and maximum intensity projection of short-axis, 2-chamber, and 4-chamber views. Each identified lesion was examined using maximum-intensity-projection and multi-planar reconstruction techniques along multiple longitudinal axes and in the transverse plane. We analyzed plaque characteristics on a per-segment basis according to a 16-segment coronary artery tree model (left main; proximal, mid and distal left anterior descending artery (LAD); first and second diagonal branches of the LAD; proximal and distal left circumflex artery; first and second obtuse marginal branches of the left circumflex artery; proximal, mid and distal right coronary artery; posterior descending artery; and left and right posterolateral branch).20)23)
Coronary artery stenosis was defined as presence of any plaque. Obstructive stenosis was defined when coronary artery segments exhibited plaque a luminal diameter stenosis ≥50%, and non-obstructive stenosis was defined when coronary artery segments exhibited plaque with a luminal diameter stenosis <50%. An individual with NCP was defined as presence of coronary stenosis, but CACS of 0.
Risk factor assessment and stratification
The baseline risk factors of coronary atherosclerosis were considered confounding variables, as previously described.22) Basic demographic data for asymptomatic subjects was acquired from a database maintained by the SNUBH health promotion center. Medical history of hypertension, diabetes mellitus, cardiovascular disease, angina, current medication profile, and smoking status were systematically acquired. Height, body weight, and blood pressure were measured during their visit. Total cholesterol, triglyceride, high density lipoprotein-cholesterol (HDL-C), low density lipoprotein-cholesterol (LDL-C), fasting plasma glucose, glycated hemoglobin, blood urea nitrogen (BUN), and creatinine level were measured after at least a 12 hours fasting period on the same day of the study. Hypertension was defined as a self-reported history of hypertension and/or use of anti-hypertensive medication, or a blood pressure ≥140/90 mm Hg. Diabetes mellitus was defined as a self-reported history of diabetes and/or receiving anti-diabetic treatment, or a fasting plasma glucose ≥126 mg/dL. We categorized all subjects into three risk groups according to the revised National Cholesterol Education Program (NCEP) guidelines: high-risk {history of coronary heart disease (CHD), CHD risk equivalents, or 10-year risk >20%}, moderate-risk (more than 2 risk factors and 10-year risk >20%), and low-risk group (0 to 1 risk factor).24)
Patient follow-up
To assess prognosis of individuals with NCP, we selected age, gender, CCTA date (±7 days)-matched controls among the subjects without NCP. If there are more subjects who meet the matching criteria, the matched-control subject was randomly selected among the qualified subjects. Matching was performed by the Medical Research Collaborating Center at Seoul National University Hospital.
After the matching group was selected, follow-up for events was performed by a dedicated physician and/or research nurse blinded to the CCTA results. Ascertainment of events was performed by telephone contact and/or review of medical records. The primary end-point was all-cause death and the secondary outcome was the composite outcome of cardiac death, non-fatal myocardial infarction (MI), unstable angina (UA) requiring hospitalization, and revascularization after 90 days of index CCTA. We only considered revascularizations more than 90 days after CCTA as outcome events to exclude downstream revascularization procedures related to index CCTA.25-27)
Statistical analysis
Continuous variables are expressed as means±1 standard deviation, whereas categorical variables are presented as frequencies. Differences between continuous variables were analyzed by Student's unpaired t-test and those between categorical variables by the chi-square test or Fisher's exact test, as appropriate. In addition, to compare differences of continuous variables and categorical variables between matched controls and patients, paired t-test and McNemar test were performed.
Univariable and multivariable binary logistic regression analyses were performed to determine association of standard risk factors and NCP. In the analysis, we selected standard risk factors as follows: age, gender, current cigarette smoking status, body mass index (BMI), disease status of hypertension, diabetes mellitus. The covariates-adjusted odds ratios (OR) and their 95% confidence intervals (CI) were derived in multiple logistic regression models. Null hypotheses of no difference were rejected if p were less than 0.05 or, equivalently, if the 95% CIs of OR estimates excluded 1. All analyses were performed with Statistical Package for the Social Sciences (SPSS) 13.0 statistical package (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics by plaque characteristics
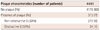
The distribution of individuals according to plaque severity was described in Table 1. Among 4491 of overall individuals without CAC, 313 subjects (7%) had coronary plaques: 279 patients (6%) with non-obstructive plaque and 34 (1%) with obstructive plaque. Among the subjects with obstructive plaque, 30 subjects (88%) were 1-vessel diseases (VD), 1 subject (3%) was 2-VD, and 3 subjects (9%) were left main disease. There is no subject with obstructive 3-VD.
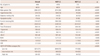
The main clinical characteristics of study subjects without CAC according to plaque characteristics were listed in Table 2. Overall, the study population consisted of 4491 individuals without CAC: 57% were male with a mean age was 48±8 years. Subjects with NCP were generally older, male, and with a higher prevalence of hypertension, diabetes, and dyslipidemia (all p<0.001). Subjects with NCP also had higher BMI, triglyceride, LDL-C, BUN, creatinine level, but lower HDL-C level compared to those without NCP. Furthermore, individuals with NCP had a higher NCEP-ATP III risk (p<0.001): only 55% of individuals with NCP were categorized as low risk according to NCEP risk stratification category while 73% of individuals without NCP were categorized as low risk.
Association of clinical risk factors with prevalence of non-calcified plaque
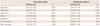
In univariable binary logistic regression analyses, age, male gender, hypertension, diabetes, dyslipidemia, current smoking, and BMI were associated with presence of NCP (Table 3). In multivariable logistic regression analyses, age (OR 1.04, 95% CI 1.02-1.05, p<0.001), male gender (OR 3.24, 95% CI 2.38-4.41, p<0.001), hypertension (OR 1.35, 95% CI 1.00-1.82, p=0.049), diabetes (OR 1.67, 95% CI 1.13-2.46, p=0.010), and dyslipidemia (OR 1.67, 95% CI 1.05-2.66, p=0.032) were independent risk factors for NCP in a model including age, gender, hypertension, diabetes, dyslipidemia, current smoking, and BMI.
Midterm outcome of individuals with non-calcified plaque
During the median follow-up duration of 22 months (25th to 75th percentile: 18 to 28 months), there is no all-cause death in subjects with NCP group (n=313) nor in age, sex, and CCTA date matched control subjects (n=313) (Table 4). For composite outcome of cardiac death, non-fatal MI, UA requiring hospitalization, and revascularization after 90 days from index CCTA, no event was reported in either group. All revascularization procedures (n=4) during follow-up period were performed within 90 days of the index CCTA.
Discussion
In a large series of individuals with CACS of zero undergoing CCTA, age, male gender, diabetes, hypertension, and dyslipidemia were independent predictors of NCP. We also observed a negligible future cardiac risk of exclusive NCP in middle aged asymptomatic subjects.
Prevalence and risk factors of non-calcified plaque
The prevalence of any NCP (>0%) was 6.2% and obstructive NCP (≥50%) was 0.7% in subjects with zero CACS. The prevalence of NCP in subjects with zero calcium in previous studies was varied. Cheng et al.28) showed prevalence of detectable NCP was 6.5% (27/416) (6.0%, non-obstructive; 0.5%, obstructive) in low to intermediate risk patients (80% of patients had chest pain or dyspnea). Akram et al.13) reported that 8.2% (4/49) had obstructive NCP in symptomatic patients, but no asymptomatic subjects (0/76) had obstructive NCP. However, Ergün et al.14) reported higher prevalence of NCP compared to the current study: 17% (54/320) had NCP and 3% (10/320) had obstructive NCP in asymptomatic subjects. Rubenstein et al.15) also found 14% (25/125) of symptomatic patients with zero calcium had NCP. The discrepancy of the prevalence of NCP might originate from the difference in pretest probability of coronary artery disease (CAD) and ethnicity of study population. We believe that the accuracy study of CCTA using ICA as a standard test by Cademartiri et al. provided a good reference of the prevalence of NCP. The prevalence of obstructive NCP in zero calcium demonstrated at CAG was 1.4% (1/71) in asymptomatic subjects which was similar to current study (0.7%).
To our knowledge, there is no study that evaluated risk factors for NCP in an asymptomatic population with zero CACS. Multivariable logistic regression analyses identified old age, male gender, diabetes, hypertension, and dyslipidemia as independent risk factors for NCP in asymptomatic population with zero calcium in current study. Therefore, it should be noted that individuals with old age, male gender, diabetes, hypertension, and dyslipidemia have a higher risk of NCP although they have zero CACS in clinical practice.
Prognosis of non-calcified plaque in individuals with zero coronary artery calcium score
In patients with suspected CAD van Werkhoven et al.18) found that NCP was independent predictor with an incremental prognostic value to CACS. Motoyama et al.17) also showed that low-attenuation plaque on CCTA was a risk factor for future acute coronary syndrome in patients with suspected or known CAD. However, there is lack of study that analyzed the prognosis of NCP in asymptomatic population with zero CACS.
The current study clearly demonstrated a negligible risk of exclusive NCP in subjects with zero CACS. During the median follow-up duration of 22 months (interquartile percentile: 18 to 28 months), there was no cardiac event in the NCP group nor even in the control group without NCP. This indicates that a CACS of zero successfully discriminates the future risk of cardiac events in asymptomatic population. Recently, the results from international multicenter CCTA registry showed that CCTA barely added prognostic value over CACS in population without chest pain syndrome.29) The results of the current study, which showed fairly good prognosis in an asymptomatic population with zero CACS, would be able to explain why CCTA failed to show significant added prognostic value over CACS.
Another important reason why CCTA failed to stratify future risk of NCP in asymptomatic subjects with CACS of zero is that the pretest probability of CAD in the current study population is low. Although 4491 subjects with no CAC were included in current analyses, the subjects with NCP were only 7% (313 subjects). Moreover, a follow-up duration of 22 months might not be enough to discriminate future risk of NCP in the current asymptomatic population. Therefore, future studies with longer follow-up and a larger population might prove the prognostic value of NCP identified by CCTA for risk prediction in this low-risk population with zero CACS.
However, CCTA has potential hazards including radiation exposure and intravenous use of contrast agent. Further, additional costs related to CCTA must be considered. Therefore, for present, the application of CCTA to detect NCP for risk stratification purpose in an asymptomatic population with CACS of zero should not be justified.
Study limitation
This study is not without limitations. We retrospectively looked at a population who underwent CCTA in a health promotion center on a self-referral basis. Therefore, selection bias could influence the results. In addition, the influence of post-test medical treatments, coronary intervention within 90 days, or risk factor control was not considered. Further, we used a 90 day window period to exclude downstream revascularization procedures related to CCTA. Thus, a revascularization procedure which was performed within 90 days from CCTA, but not a downstream procedure might be excluded from the clinical outcome. Moreover, the topographic distribution of coronary plaques, and various plaque assessment approaches including area stenosis, minimal lumen diameter, and minimal lumen area were not included in current analyses.

 XML Download
XML Download