

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Early statin therapy has become the standard of care in patients with acute coronary syndrome (ACS).1-4) However, the great majority of clinical trials have excluded patients with impaired hemodynamics, particularly cardiogenic shock (CS), which is the most common cause of death following acute myocardial infarction (MI) with high short-term mortality ranging from 42 to 48 percent.5)6) The present study was conducted to investigate the effect of early statin treatment on a 12-month clinical outcome in CS patients with acute MI undergoing revascularization therapy.
Subjects and Methods
Study population and data collection
The Korea Acute Myocardial Infarction Registry (KAMIR) is the first nationwide, multicenter data collection registry in Korea, designed to track the outcomes of patients presenting with acute MI.7)8) Since its launch in November 2005, the KAMIR included 51 community and teaching hospitals and contained data on 14870 patients through January 2008.
The study population was derived from patients enrolled in the KAMIR between November 2005 and January 2008. We included 616 patients (18 years of age or older) presenting with acute MI complicated with CS who underwent revascularization therapy either with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). From this population, we excluded 53 patients who had been on statin treatment before the onset of acute MI and 10 patients who received non-statin lipid lowering therapy during admission. A total of 553 patients were selected and divided into 2 groups: those who received statin treatment during hospitalization (n=280) and those who did not (n=273). Atorvastatin was used in 41% of the patients (10 mg in 69%, 20 mg in 17%, 40 mg in 14%), pravastatin in 39% (40 mg in 92%, 20 mg in 4%, 10 mg in 4%), rosuvastatin in 9% (10 mg), simvastatin in 6% (20 mg in 75%, 10 mg in 25%), pitavastatin in 4% (2 mg), and fluvastatin in 1% (80 mg), respectively. We defined "early" treatment as statin therapy instituted during hospitalization whether it was before or after revascularization therapy. Statin was started on admission in 60%, within 24 hours in 21%, on day 2 in 9%, on day 3-4 in 6%, and on days 5-12 in 4%, respectively. Statin was administered before PCI or CABG in 52% of the patients.
The diagnosis of acute MI was based on a clinical presentation consistent with acute MI and at least 1 of the following: specific electrocardiographic changes, serial increases in serum cardiac biomarkers of myocardial necrosis, and/or angiographic documentation of coronary artery disease. For the purpose of the present study CS was defined as the presence or development of Killip class IV heart failure.
The present study was conducted according to the Declaration of Helsinki. The institutional review board of all participating centers approved the study protocol. The approval number was 05-49 of Chonnam National University Hospital. Written informed consent was obtained from all participating patients.
Study endpoints and definitions
Twelve-month major adverse cardiac events were defined as the occurrence of major adverse cardiac events, defined as death from any cause, recurrent MI, or repeat revascularization within 12 months after admission. Recurrent MI was defined as the recurrence of symptoms or the presence of electrocardiographic changes in association with a rise in cardiac biomarker levels above the upper limit of normal. Repeat revascularization was defined as any repeat surgical or percutaneous intervention, including revascularization procedures performed to treat segments not treated in the index procedure.
Statistical analysis
Baseline differences between the 2 groups were compared using either the t-test or the Mann-Whitney U test for continuous variables and the chi-square test or Fisher's exact test for categorical variables. Unadjusted hazard ratios (HR) and their 95% confidence intervals (CI) were calculated for outcome variables using Cox regression analysis. Since receiving statin treatment was not randomly assigned in this study population, we used propensity score matching to adjust for potentially confounding factors and selection biases.9)10) We performed a one-to-one matched analysis without replacement on the basis of the estimated propensity score of each patient. For each patient, a propensity score for the likelihood of receiving statin therapy at admission was calculated by forward logistic regression analysis and included 63 variables of clinical and procedural characteristics, procedural complications, and medical treatment during hospitalization shown in Table 1 and 2. The c-statistic for the propensity score derivation model was 0.84, indicating a strong ability to discriminate between the two groups. Using the estimated logits, we first randomly selected a patient in the group receiving statin and then matched the patient to the closest patient in the group not receiving statin. Patients in the group not receiving statin who had an estimated logit within a standard deviation of 0.6 of the selected patients in the group receiving statin were eligible for matching. We selected 0.6 because this value has been shown to eliminate approximately 90% of the bias in observed confounders.11) We were successfully able to match 200 patients receiving statin to 200 patients not receiving statin at admission. Differences between matched pairs were evaluated using the paired t-test or the Wilcoxon signed rank test for continuous variables and the McNemer test for categorical variables. The risks of clinical end points in the matched cohort were compared by the use of Cox regression models stratified on matched pairs. To identify independent predictors of the 12-month clinical outcome (composite of death, MI, repeat revascularization), multivariate Cox proportional hazards regression analysis was performed including 14 variables with univariate p<0.01 given the number of events per confounder: age, male gender, smoking, previous stroke, ventricular tachycardia/fibrillation at presentation, smoking, high-sensitivity C-reactive protein, left main culprit lesion, lesion type B2/C, post-PCI Thrombolysis in Myocardial Infarction (TIMI) grade 3, use of aspirin, clopidogrel, beta-blockers, and angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB). The regression analysis was done using backward stepwise selection and variables were removed if p>0.10. A 2-sided p<0.05 was considered statistically significant. Statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS) 17.0 (SPSS Inc., Chicago, IL, USA) and Stata 11.0 (Stata Corp., College Station, TX, USA).
Results
Baseline characteristics of patients with and without statin treatment during hospitalization are shown in Table 1. Patients who received statin were younger, had chest pain more often, and were less likely to have severe hemodynamic instability and left ventricular (LV) dysfunction. They had higher levels of total and low density lipoprotein-cholesterol and lower levels of glucose at admission. Statin-treated patients were less likely to have left main disease and had a higher rate of post-PCI TIMI 3 flow and a lower rate of periprocedural complications. Also, they had complex lesions more often, underwent coronary stenting, and received antiplatelet and adequate anti-ischemic medications (Table 2). After propensity score matching, the major differences in baseline clinical characteristics and proportion of procedures, complications, and medical treatment during hospitalization were minimized or eliminated (Table 3 and 4).
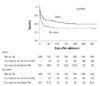
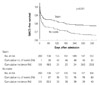
Unadjusted and adjusted clinical outcomes within 12 months after admission are summarized in Table 5 and 6. Among the 273 patients without statin treatment, the unadjusted in-hospital mortality was 43.2% compared to 12.9% among the 280 patients with statin treatment (p<0.001). After propensity score matching, patients who did not receive statin still exhibited higher in-hospital mortality than those who received statin (17.0% vs. 29.5%, p=0.002). The unadjusted 12-month mortality and composite major adverse cardiac events were significantly higher in patients without statin treatment (45.4% vs. 18.9%, p<0.001 and 50.9% vs. 24.6%, p<0.001, respectively). In the propensity score-matched cohort, Cox regression analysis stratified on matched pairs showed that statin treatment during hospitalization was significantly associated with a reduction in 12-month mortality (23.0% vs. 32.5%; HR, 0.53; 95% CI, 0.35-0.82; p=0.004) and composite major adverse cardiac events (25.5% vs. 40.0%; HR, 0.44; 95% CI, 0.29-0.66; p<0.001) (Figs. 1 and 2). On multivariate analysis, factors associated with a reduction in 12-month death/MI/repeat revascularization were post-PCI TIMI flow 3 (HR, 0.53; 95% CI, 0.37-0.77; p=0.001), use of statin (HR, 0.53; 95% CI, 0.38-0.74; p<0.001), ACEI/ARB (HR, 0.50; 95% CI, 0.35-0.74; p<0.001), and beta blockers (HR, 0.51; 95% CI, 0.35-0.74, p<0.001). Factors associated with an increase in 12-month death/MI/repeat revascularization were left main disease (HR, 2.09; 95% CI, 1.11-3.92; p=0.022), previous stroke (HR, 2.06; 95% CI, 1.23-3.44; p=0.006), and older age (>65 years) (HR, 1.10; 95% CI, 1.004-1.033, p=0.013).
Discussion
Early statin therapy has become recommended as a standard treatment in patients with ACS,1-4) and a number of clinical trials have supported the initiation of statin therapy before discharge after ACS.12-17) However, most clinical trials have excluded CS patients, and little data is available on the benefit of statin in patients with CS complicating acute MI. The present study suggested that early statin treatment during hospitalization improved in-hospital survival as well as the 12-month clinical outcome in CS patients with acute MI undergoing revascularization therapy. One finding of note in our study is that statin therapy was associated with reduced in-hospital mortality. There have only been a few studies on the survival benefit of statin therapy very early in the course of ACS. Two series of observational studies from the National Registry of Myocardial Infarction 4 (n=174635; 2270 CS patients)14) and the Global Registry of Acute Coronary Events (n=15481; 186 CS patients)18) revealed that the use of statin therapy during hospitalization for ACS was associated with a significantly lower rate of in-hospital mortality: 3.9% vs. 8.6%, p<0.001 and 2.1% vs. 9.9%, p<0.001, respectively. Garot et al.19) investigated the early beneficial effect of statin therapy in patients undergoing PCI for acute ST-elevation MI complicated by CS. Patients undergoing statin therapy at the time of PCI (n=30) had significantly lower in-hospital mortality than those without statin therapy (n=81) {46.7% vs. 70.4%; odds ratio (OR), 0.35; 95% CI, 0.15-0.88; p=0.026}. Schmidt et al.20) observed that patients suffering multiple organ dysfunction syndrome (MODS) treated with statin (n=40, cardiovascular causes 93%) had significantly lower in-hospital mortality than age- and sex-matched MODS patients not treated with statin (n=80) (35% vs. 72%, p<0.0001). Suggested mechanisms by which statin therapy may influence early mortality in patients with MODS included modulation of inflammatory responses through enhanced expression of endothelial nitric oxide synthase and reduced polymorphonuclear leukocyte-endothelium interactions,21) and an increase in vagal activity, which prevents a spillover of proinflammatory products into the circulation.22-24) Merx et al.25)26) reported that statin treatment improved survival in a murine model of sepsis-induced hemodynamic alterations. As with pretreatment with simvastatin,25) mice treated 6 hours after onset of sepsis with atorvastatin, pravastatin, or simvastatin demonstrated preservation of cardiac function and hemodynamic stability.26) Improved susceptibility to endothelial nitric oxide synthase stimulation and reduced endothelial adhesion of leukocytes were proposed as underlying mechanisms. In an observational study by Almog et al.27) on 361 patients with acute bacterial infection, prior statin therapy was associated with a reduced rate of severe sepsis (OR, 0.07; 95% CI, 0.01-0.51; p=0.01). More recently, Hackama et al.28) also showed in a matched-pair analysis on 141487 patients with cardiovascular disease that statin therapy at both high and low doses was associated with a considerably lower rate of fatal sepsis (OR, 0.75; 95% CI, 0.61-0.93). In a similar manner, in patients with CS complicating acute MI, the use of statins combined with timely revascularization may provide a potential survival benefit through modification of the heightened systemic inflammation, which may primarily manifest as an increase in early mortality frequently in association with severe myocardial ischemic insult, refractory heart failure, and malignant ventricular arrhythmia. This mortality-reducing cardioprotective effect of statins needs to be confirmed in appropriately powered randomized clinical trials.
Our analysis has several limitations. First, although these results come from a large cohort and adjustment was performed using propensity score analysis for a large number of confounding variables, unmeasurable factors may still exist. Second, the distinction between CS caused by LV failure and other etiologies such as predominant right ventricular shock or mechanical complications was not possible. Finally, we could not assess the effect of specific types of statins, dosages, or timing of statin treatment (i.e., before or after PCI or CABG) on observed outcomes.
In conclusion, in statin-naive CS patients with acute MI undergoing revascularization therapy, early statin treatment initiated during hospitalization was associated with lower in-hospital mortality and a reduction in major adverse cardiac events at a 12-month follow-up. Additional research is warranted to elucidate the pathophysiologic mechanisms for the benefit of early statin use in this highest risk subset of patients with acute MI.






 XML Download
XML Download