

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Wolff-Parkinson-White (WPW) syndrome is characterized by ventricular pre-excitation that ventricles are electrically and mechanically pre-excited through an accessory pathway, which connects atria and ventricles. Supraventricular tachycardia is frequently associated with symptomatic WPW syndrome in clinical practice. A rare cause of morbidity in infants and children with WPW syndrome is left ventricular (LV) dysfunction or dilated cardiomyopathy (DCM), which may attribute to the recurrent or incessant tachycardia.1)2) Recently however, several small case series and case reports suggested a possible association between accessory pathways and ventricular dysfunction in the absence of sustained tachyarrhythmias.3-11) The eccentric premature ventricular activation via an accessory pathway results in an asynchronous spread of ventricular depolarization and this asynchronous ventricular activation may provoke ventricular dysfunction.12) The occurrence of ventricular dysfunction in asymptomatic WPW syndrome may depend on the location of the accessory pathway, and invariably it was reported the electrophysiological features was the right sided accessory pathway, especially in the septal or paraseptal location.7)10) It is thought that this type of accessory pathway induces abnormal interventricular septal wall motion leading to LV dyssynchrony and subsequently ventricular dysfuction or DCM through LV remodeling. This non-tachycardia type of LV dysfunction with WPW syndrome is characterized by complete recovery of the ventricular function after ablation or spontaneous regression of pre-excitation. It is the purpose of this article to review the clinical and electrophysiologic evidence for this association and to discuss the underlying pathophysiological mechanism.
Go to : 
Occurrence of Left Ventricular Dysfunction and Dilated Cardiomyopathy in the Asymptomatic Wolff-Parkinson-White Syndrome
The prevalence of LV dysfunction associated with WPW syndrome in the absence of tachyarrhythmias is unknown. Age distribution of these patients with pre-excitation related LV dysfunction is wide, ranging from infants to old age. In 1998 Yamanaka et al.3) suggested the association between LV dysfunction and WPW syndrome for the first time in a 67 year old man with type B WPW syndrome, of whom cardiac function improved after catheter ablation. Several years thereafter, in 2004 Emmel et al.4) described the improvement of ventricular function after the disappearance of pre-excitation in 4 children with DCM associated with WPW syndrome, and suggested a causal relationship between ventricular pre-excitation and DCM. Thereafter, only several small case series and case reports have been reported until now and summarized in Table 1. However, the incidence of this association might have been underestimated. Some patients with abnormal wall motion might have undergone an electrophysiological study and catheter ablation before overt ventricular dysfunction developed. It is also possible that some patients have been considered only to have idiopathic DCM coincidentally.
Go to :
Wall Motion Abnormalities in Wolff-Parkinson-White Syndrome
Patients with manifested antegrade accessory pathway conduction have asynchronous ventricular wall motion because of abnormal impulse propagation by premature eccentric ventricular activation over a bypass tact. Systolic and diastolic wall motion abnormalities have been well described in WPW syndrome. It was found in the earlier echocardiographic studies13-16) that the pattern of abnormal ventricular contraction was dependent on the location of the accessory pathway. Left-sided accessory pathways produced premature anterior motion in the posterior LV wall and right-sided accessory pathways showed abnormal interventricular septal motion. Left-sided accessory pathways producing typical anterior motion of the LV posterior wall is visible on M-mode echocardiography in early systole as a small, distinct bump and this unopposed early contraction of the posterior wall results in abnormal anterior motion of the interventricular septum. The right-sided accessory pathway related abnormal interventricular septal motion consists of an early systolic posterior and subsequent midsystolic anterior motion, with a delay in the usual late systolic septal movement. These abnormal septal motions in type B WPW syndrome are similar to those described in patients with left bundle branch block (LBBB). Grines et al.17) observed abnormal interventricular septal motion in patients with LBBB and this abnormal septal motion in LBBB corresponded to periods of asynchrony in contraction, ejection, end systole, and end diastole between the right and left ventricle. They also found that regional ejection fraction of the septum decreased in LBBB compared with that of normal subjects and this loss of septal contribution resulted in a reduction in global ejection fraction in LBBB compared to normal subjects.
In the earlier echocardiographic studies, they observed that abnormal septal motion was normalized after loss of pre-excitation in patients with type B WPW syndrome and suggested that abnormal septal motion is related to the altered sequence of ventricular activation during pre-excitation.14)15)
Go to :
Left Ventricular Dysfunction and Dilated Cardiomyopathy and Location of Accessory Pathway
Several recent studies suggested that WPW syndrome may lead to regional and global contractile dysfunction resulting from aberrant impulse propagation.5)9)10)12) The right septal and paraseptal accessory pathways have been considered the main location to induce LV dysfunction. Tomaske et al.7) showed in 56% of patients with right septal or posteroseptal accessory pathways, LV ejection fraction decreased and septal-to-posterior wall motion delay increased. They discussed the importance of septal and posteroseptal location of accessory pathways to cause ventricular dysfunction. The extent of the pre-excited ventricular myocardium depends on the relative timing of normal and eccentric ventricular activation. In left free wall pathways, the amount of pre-excited myocardium is rather small because of long conduction time from the sinus node to the atrial pathway insertion leading to almost normal activation of the left ventricle via atrioventricular nodal conduction. In right free wall pathways, LV activation is almost synchronous over the normal conduction pathway, with a precontraction area being limited to the right ventricular free wall. In contrast to right free wall pathways, septal and posteroseptal pathways may induce earlier interventricular activation, subsequently substantial part of septal pre-excitation and delayed activation of LV free wall.
Early septal activation may induce paradoxical or hypokinetic interventricular septal motion, similar to septal motion abnormalities seen in patients with right ventricular pacing or LBBB, and this dyskinetic segment may function like an aneurysm and induce adverse remodeling with progressive dilation. The detrimental effect of chronic right ventricular pacing or LBBB on LV function has been well described. Chronic asynchronous electric activation in the patients with LBBB or right ventricular pacing disturbs the myocardial regional workload and wall stress, which may result in abnormal wall motion, regional myocardial perfusion defects leading to adverse remodeling with asymmetry of wall thickness and progressive LV dilation.17-20) In an animal study,21) the abnormal impulse propagation by ventricular pacing causes considerable disturbances in regional systolic fiber shortening, mechanical work, blood flow, and oxygen consumption - and in early activated regions, the values are low.
An early activation of the basal septum via septal and paraseptal pathways will induce segmental contraction which is unopposed by the activation of the remaining left ventricle. On these early contracting segments, imposed preload will be low, resulting in decreased myocardial work and thinning of the myocardium, which is manifested as extreme systolic bulging of the pre-excited basal septum towards the right ventricle. Fig. 1 shows paradoxical systolic bulging of the basal septum in a 9-year-old girl with right anterior accessory pathway. This early basal septal segmental contraction with bulging and delayed free wall activation may lead to significant dyssynchrony in the LV motion and thereby cause ventricular dysfunction. A study using recent echocardiographic technique22) showed local ejecting shortening was impaired at the pre-excitation site and at similar electrical and mechanical dyssynchrony, WPW syndrome with septal accessory pathways had more extensive hypokinesia than did WPW syndrome with LV free wall accessory pathways. Kwon et al.9) reported that LV systolic function was reduced in all patients with septal pathways, compared to patients with left or right free wall pathways. In their study, compared to patients with normal septal motion, patients with septal dyskinesia had a reduced LV ejection fraction and an increased LV end diastolic dimension. Tomaske et al.7) also suggested that WPW syndrome with right septal or posteroseptal pathways may cause LV dyssynchrony and jeopardize global LV function. They used conventional echocardiographic and recent speckle tracking imaging techniques to see LV dyssynchrony in patients with septal accessory pathways. In these two recent studies, significant LV dyssynchrony disappeared after catheter ablation with subsequent improvement of systolic LV function. These observations support the importance of dyssynchrony in the pathogenesis of LV dysfunction associated with ventricular pre-excitation. Fig. 2 shows a heterogeneous pattern in the radial strain assessment using 2-dimensional speckle tracking echocardiography that changed into a more homogeneous pattern after catheter ablation of the right anterior accessory pathway in a 9-year-old girl with asymptomatic WPW syndrome.
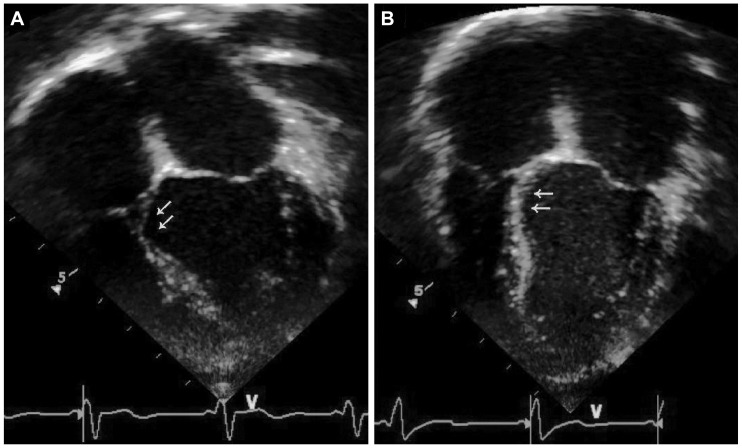 | Fig. 1Two-dimensional echocardiography in a 9-year-old girl with right anterior accessory pathway. A: bulging of basal septum with thinning (arrow) is seen in end systole prior to catheter ablation. B: paradoxical motion and bulging of basal septum (arrow) improves one month after catheter ablation.
|
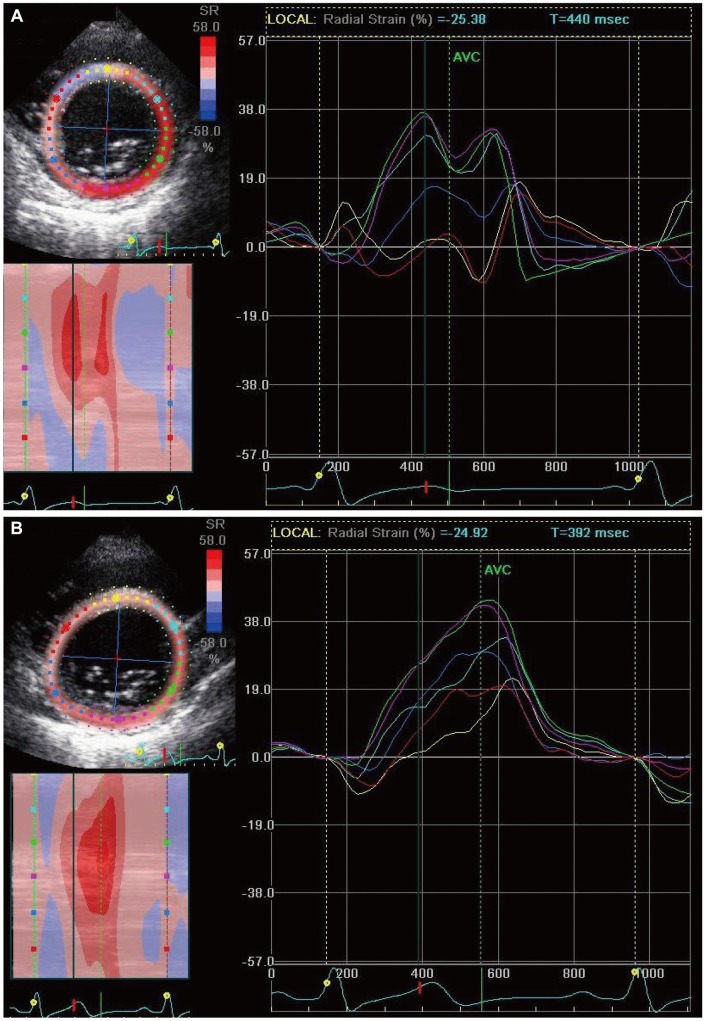 | Fig. 2Radial strain assessment using 2-dimensional speckle tracking echocardiography. In the parasternal short axis view at the level of the mitral valve of a 9-year-old girl with a right anterior accessory pathway, radial strain assessment shows an inhomogeneous pattern with paradoxical negative value at the basal septal and basal anterior wall before radiofrequency catheter ablation (A). One month after ablation, inhomogeneity in the radial strain much improves and at the basal septal and basal anterior wall the radial strain reverts to a positive value (B).
|
However, It is unknown why not all patients with right sided accessory pathways develop ventricular dysfunction, in the absence of incessant tachyarrhythmias. In 1977, Levovitz et al.16) suggested that the determinants of abnormal septal wall motions are the location, right ventricular lateral freewall or septal and degree of ventricular pre-excitation. They reported that asynchronous movement was observed only in their patients in whom duration of the QRS complex was greater than 130 msec. In the study by Kwon et al.,9) all patients with septal dyskinesia and reduced LV ejection fraction showed longer pre-excited QRS duration than those with normal septal motion. Another recent study suggested that different locations of paraseptal accessory pathways may induce a variable degree of LV dyssynchrony and dysfunction. Tomaske et al.7) reported that their patients with midseptal and anteroseptal pathways demonstrated lower LV ejection fraction and a higher degree of intraventricular LV dyssynchrony compared with those with posteroseptal pathways. The degree of pre-excitation and the degree of dyssynchrony induced by the different location of the accessory pathway may be the additional factor for development of ventricular dysfunction in these patients.
Go to :
Prognosis of Left Ventricular Dysfunction or Dilated Cardiomyopathy Related with Accessory Pathway
The prognosis of accessory pathway induced LV dysfunction or DCM is excellent. In the reported cases shown in Table 1, cardiac function improved and normalized acutely or within several months after loss of pre-excitation, either spontaneously or by catheter ablation or appropriate medical therapy. These findings suggest that recovery of ventricular function through LV reverse remodeling occurs after loss of ventricular pre-excitation. In infants and small children, catheter ablation is chosen as a last alternative therapy due to its higher risk of complications and uncertain long-term effect of ablation scars on young myocardium.23)24) Cadrin-Tourigny et al.6) reported severe LV dysfunction in two young infants with asymptomatic WPW syndrome and in both infants, successful pharmacologic suppression of posteroseptal accessory pathway conduction with amiodarone resulted in dramatic improvement in LV function. It further supports the pathogenic association of accessory pathway with LV dysfunction or DCM. Therefore, accessory pathway associated ventricular dysfunction should be suspected in all patients presenting with DCM and ventricular pre-excitation, especially with right sided accessory pathways, when tachyarrhythmias induced ventricular dysfunction is ruled out. However, many asymptomatic patients with WPW and septal and paraseptal accessory pathways may have abnormal ventricular wall motion without overt ventricular dysfunction or DCM and the catheter ablation of accessory pathways in these patients is still controversial. It seems reasonable that catheter ablation should be reserved for those patients in whom progression of adverse LV remodeling and deteriorating cardiac function are demonstrated in the conventional and recently developed techniques of echocardiography during follow-up.
Go to :
Conclusion
The causal relationship between LV dysfunction or DCM and WPW syndrome in the absence of tachyarrhythmias is recently recognized. Right-sided accessory pathways may induce LV dyssynchrony, leading to adverse remodeling and ventricular dysfunction. The prognosis of these patients is excellent. Loss of ventricular pre-excitation spontaneously or by catheter ablation results in mechanical resynchronization, reverse remodeling and LV function recovers completely.
Go to :
 XML Download
XML Download