

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Fibrate is a peroxisome proliferator-activated receptor α agonist and is widely used to decrease triglyceride and to increase high density lipoprotein-cholesterol (HDL-C).1) Several large-scale studies have investigated the effect of fibrate in the prevention of cardiovascular events.2-6) However, the results are contentious. Inflammatory processes play an important role not only in the pathogenesis of atherosclerosis but also in the occurrence of acute coronary syndromes.7) C-reactive protein (CRP) is a prototype of inflammatory markers and high levels of CRP are associated with an increased risk for cardiovascular diseases.8) Several studies have investigated the effect of fibrate on CRP levels.9-25) However, most studies had limitations in the study design and the results were inconsistent. In addition, most studies enrolled too few patients for subgroup analysis. The aims of this study were to evaluate the effect of fenofibrate on CRP levels in hypertriglyceridemic patients compared with that of the well-matched comparison group and to explore variables affecting CRP levels in a relatively large number of patients.
Subjects and Methods
This retrospective case-control enrolled 280 patients with a triglyceride level ≥200 mg/dL. Exclusion criteria were 1) new onset diseases that influence lipid levels, such as diabetes mellitus, infectious diseases, or other endocrinologic diseases within 3 months, 2) aspartate aminotransferase or alanine aminotransferase levels ≥3-fold the upper normal limit, 3) medications within 3 months that affect lipid levels, and 4) baseline and follow-up CRP levels ≥10 mg/L. Patients were divided into two groups: the comparison group was managed with general measures (n=140) and the fenofibrate group was treated with 200 mg of fenofibrate (n=140). General measures included a low-calorie and a low-fat diet and aerobic exercise. A part of these data was published previously.23)
Concentrations of CRP and lipids were measured before and after management for 2 months. After overnight fasting, blood samples were obtained. Concentrations of total cholesterol and triglyceride were determined by the enzymatic method using an automatic analyzer (Model 7150, Hitachi, Tokyo, Japan). The concentration of HDL-C was measured by the direct method using an automatic analyzer. The concentration of high sensitivity CRP was determined by nephelometer method using an N High Sensitivity CRP kit (Dade Behring Marburg GmbH, Marburg, Germany).
Data are expressed as mean±SD. Statistical analysis was performed using the Social Package for the Social Sciences (SPSS V9.0K, SPSS Inc., Chicago, IL, USA). For CRP and triglyceride, the Wilcoxon signed-rank test was used to compare concentrations before and after therapy, and the Mann-Whitney U test was used to evaluate differences between groups. For other variables, the paired t-test was used to compare the concentrations before and after medication, and Student's t-test was used to evaluate differences between groups. CRP and triglyceride were log-transformed and the relationships between parameters were analyzed using Pearson's correlation method. Stepwise linear regression method was used to obtain independent variables. The distribution of discrete variables was analyzed using the χ2 test. Two-tailed null hypotheses of no difference were rejected if p were less than 0.05.
Results
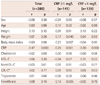
Baseline demographic and clinical characteristics were similar between the two groups except for the number of patients with diabetes mellitus (p=0.032). Baseline CRP levels and lipid profiles were also similar (Table 1).
C-reactive protein levels decreased in both the fenofibrate (from 1.53±1.58 to 1.29±1.44 mg/L, p=0.003) and comparison (from 1.54±1.70 to 1.40±1.44 mg/L, p=0.048) groups (Table 2). Changes in CRP levels were not significantly different between the two groups (-0.24±1.56 mg/L vs. -0.14±1.69 mg/L, p=0.27). In all patients (n=280), CRP levels decreased more in patients with higher baseline CRP levels than in those with lower levels (r=-0.47, p<0.001) (Table 3, Fig. 1). Fenofibrate increased HDL-C level (p=0.000) and decreased total cholesterol (p=0.026), nonHDL-C (p=0.000), and triglyceride (p=0.000) levels compared with the comparison group. There were no significant changes in low density lipoprotein-cholesterol levels (p=0.81) between the two groups.
In patients with a baseline CRP level ≥1 mg/L, CRP levels decreased in both the fenofibrate (n=69, from 2.55±1.73 to 1.76±1.74 mg/L, p=0.000) and comparison (n=72, from 2.49±1.92 to 1.83±1.36 mg/L, p=0.001) groups (Table 2). CRP levels fell more in the fenofibrate group than in the comparison group (-0.79±1.90 mg/L vs. -0.66±1.77 mg/L, p=0.025). In these patients (n=141), CRP levels decreased more in patients with higher baseline CRP levels (r=-0.29, p=0.001) (Fig. 1), lower body mass index (BMI, r=0.23, p=0.007) (Fig. 2), fenofibrate therapy (r=0.19, p=0.025), and lower body weight (r=0.17, p=0.040) (Table 3). Among these variables, higher baseline CRP levels, lower BMI, and fenofibrate therapy were independent in the stepwise linear regression analysis. The association of changes in CRP levels with BMI was found only in the fenofibrate group (r=0.28, p=0.022) and not in the comparison group (r=0.17, p=0.15) (Fig. 2). In patients with a baseline CRP level <1 mg/L, CRP levels did not change in both the fenofibrate (n=71, p=0.11) and comparison (n=68, p=0.20) groups (Table 2).
In all patients (n=280), baseline CRP levels were higher in patients with a BMI >26 kg/m2 than in those with a BMI ≤26 kg/m2 (1.63±1.54 mg/L vs. 1.47±1.71 mg/L, p=0.014). However, when patients with a baseline CRP level <1 mg/L were excluded, there were no significant differences between the two groups (2.37±1.64 mg/L vs. 2.67±1.98 mg/L, p=0.59). In patients with a CRP level ≥1 mg/L and a BMI ≤26 kg/m2, CRP levels decreased in both the comparison and fenofibrate groups (p=0.004 and p=0.000, respectively) and more in the fenofibrate group than in the comparison group with a borderline significance (-1.21±1.82 mg/L vs. -0.89±1.92 mg/L, p=0.097) (Table 2). In patients with a baseline CRP level ≥1 mg/L and a BMI >26 kg/m2, CRP levels tended to decrease in both groups (p=0.064 and p=0.057, respectively). However, these changes were not significantly different between the two groups (p=0.63).
In patients with a baseline HDL-C level <40 mg/dL, CRP levels decreased in the fenofibrate group (n=83, p=0.006) and not in the comparison group (n=79, p=0.12) (Table 2). However, changes in CRP levels were not significantly different between the two groups (-0.30±1.42 vs. -0.17±1.83, p=0.41). In patients with a baseline HDL-C level ≥40 mg/dL, CRP levels did not change in both the fenofibrate (n=57, p=0.15) and comparison (n=61, p=0.27) groups.
Discussion
The present study demonstrated that fenofibrate had a small but a significant anti-inflammatory effect in hypertriglyceridemic patients with high risk for cardiovascular diseases and not severely overweight. To our knowledge, this is the first report to evaluate the effect of fibrate on CRP levels by baseline CRP levels and obesity.
In the present study, patients with diabetes mellitus were included more in the fenofibrate group than in the comparison group (p=0.032). Patients with diabetes mellitus had higher CRP levels than those without diabetes mellitus (2.44±2.23 mg/L vs. 1.37±1.45 mg/L, p=0.001).26) However, changes in CRP levels were not different (0.34±2.08 mg/L vs. 0.22±1.40 mg/L, p=0.35) in the fenofibrate group and the number of patients with diabetes mellitus was relatively small (n=29). Therefore, we believe that this difference did not influence the results.
In all patients, CRP levels decreased in both the comparison and fenofibrate groups. However, changes in CRP levels were not significantly different between the two groups. This finding suggests that the reduction of CRP levels was not by fenofibrate therapy but by general measures.
As changes in CRP levels were closely associated with baseline CRP levels, we divided patients into two subgroups according to a median value of baseline CRP levels. In patients with a CRP level ≥1 mg/L, fenofibrate decreased CRP levels more compared with general measures. This finding suggests that fenofibrate may have an anti-inflammatory effect only in patients with high risks for cardiovascular diseases.
Several studies have investigated the effect of fibrate on CRP levels.9-25) However, most studies did not have a comparison group9-11) or a comparison of fibrate with statins.12-16) In several studies with a comparison group, there were differences in the clinical characteristics and baseline CRP levels.17-19) In the present study, CRP levels decreased not only in the fenofibrate group but also in the comparison group. The reduction was more pronounced in patients with higher CRP levels than in those with lower CRP levels. Since previous studies enrolled high-risk patients with diabetes mellitus, metabolic syndrome, or dyslipidemia, baseline CRP levels were often high. Most of these studies report that fibrate markedly reduces CRP levels. Therefore, it is critical to include a well-matched comparison group to avoid false-positive results and the data from these studies must be interpreted with caution.
In well-designed studies, fibrate markedly reduced CRP levels in several studies20-22) and did not in other studies.23-25) In a retrospective analysis of the Bezafibrate Infarction Prevention (BIP) study which included 3122 patients with chronic coronary heart diseases, CRP levels increased by 3.0% in bezafibrate-treated patients and by 3.7% in the comparison group after 2 years.24) In subgroup analysis of the Fenofibrate Intervention and Event Lowering in Diabetes study which included 170 patients with diabetes mellitus, fenofibrate failed to decrease CRP levels.25) In contrast, several studies with a relatively small number of patients have reported that fibrate reduces CRP levels by 25-51%.20-22) In the present study, fenofibrate significantly reduced CRP levels in patients with a baseline CRP ≥1 mg/L, but not in all patients. The wide range of baseline CRP levels may partially explain the inconsistency of the previous studies.
We excluded patients with baseline and follow-up CRP levels ≥10 mg/L in order to rule out the possibility of inflammation from other causes.27) Most studies did not include these exclusion criteria. Very high baseline and follow-up CRP levels may overestimate and underestimate the effects of fibrate, respectively.
In earlier large-scale studies, fibrate reduced cardiovascular events in patients with high nonHDL-C levels and in patients with coronary artery diseases and low HDL-C levels.2)3) In recent studies, fenofibrate has failed to reduce the primary endpoints.4-6) However, fenofibrate consistently reduced cardiac events in a subgroup with low HDL-C and high triglyceride levels.4-6) In the BIP study, high CRP levels were associated with low HDL-C and high triglyceride levels.4) Therefore, fenofibrate may be effective only in patients who have high CRP levels. In the present study, the effect of fenofibrate was evident in patients with high baseline CRP levels. This finding suggests that baseline CRP levels may be useful to determine whether fibrate is prescribed to a patient or not. For example, statin was more cardioprotective in patients with high CRP levels than in those with low CRP levels.28) Further studies are needed to confirm this hypothesis.
The present study showed a very interesting finding that was previously unknown. The reduction of CRP level was positively associated with BMI (r=0.23, p=0.007) (Fig. 2) in patients with a baseline CRP ≥1 mg/L. Fenofibrate decreased CRP levels more in patients with a BMI ≤26 kg/m2 than in patients with a BMI >26 kg/m2, although it did not reach the statistical significance (p=0.097). This finding suggests that fenofibrate can modify the inflammatory process from the metabolic origin but not that from the obesity. It has been reported that CRP level and the effect of fibrate on it are dependent on genetic polymorphisms.29) In addition, this study showed that the obesity could also influence the effect of fibrate CRP levels.
There are several limitations in this study. This study was performed at a single hospital in Korea. Patients with diabetes mellitus were more frequent in the fenofibrate group than in the comparison group. This study enrolled an adequate number of patients for most analyses. However, the subgroup analysis according to body weight showed a borderline significance due to the small number of patients. This finding needs to be confirmed in more large scale studies.
In conclusion, the present study has shown that fenofibrate has a small but significant anti-inflammatory effect in selected high-risk patients with high inflammatory conditions and without severe overweight and/or with low HDL-C.




 XML Download
XML Download