

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Radiofrequency catheter ablation (RFCA) is widely applied as a curative treatment for many types of pediatric cardiac arrhythmias.1) The first pediatric RFCA was performed in a child with supraventricular tachycardia (SVT) in 1989.2)
We have used RFCA as a treatment for pediatric tachyarrhythmias in Daegu since 1993. Pediatric patients display atrioventricular reentry tachycardia (AVRT) as the most common tachycardia mechanism, paroxysmal attack, and tachycardia occurrence related to congenital heart disease (CHD).3-5)
In Korea, there were a few reports about pediatric electrophysiology studies (EPS) and RFCA and their characteristics.4)5) One report described sedation methods and successes, complications and recurrence rates, and another report included RFCA results in cases including congenital heart anomalies.
Although there were records of data in regional centers, we experienced more pediatric cases than previous studies therefore we performed a retrospective study to elucidate the frequency of tachycardia mechanisms and the characteristics of accessory pathways (APs) confirmed by RFCA in pediatric tachycardia. In addition, we analyzed the efficacy and safety of pediatric RFCA.
Subjects and Methods
Patient selection
Pediatric EPS and RFCA were performed in Keimyung University Dongsan Medical Center and Kyungpook National University Hospital according to the pediatric RFCA guidelines of the NASPE Expert Consensus Conference6) or by the choice of the patients and their parents, when patients had recurrent symptomatic tachycardia. After tachycardia was induced by atrial or ventricular pacing during EPS, RFCA was attempted. RFCA was not performed in patients in whom tachycardia could not be induced by EPS, and they were excluded from this study.
From August 1993 to July 2011, we performed EPS on 2000 patients at Keimyung University Dongsan Medical Center and 524 patients at Kyungpook National University Hospital. Patients ≤18 years of age at the time of the EPS and RFCA were included in the present study. Among the 2000 patients in Keimyung University Dongsan Medical Center, there were 142 pediatric patients, of whom 130 were enrolled in the present study. In Kyungpook National University Hospital, there were 151 pediatric patients, and 130 patients were enrolled in the present study. We retrospectively evaluated the electrophysiological characteristics of these 260 patients, such as tachycardia mechanism, ablation site and locations of APs, results and complications of RFCA, failure of RFCA and recurrence of arrhythmia after RFCA, by reviewing the patients' medical records.
Statistical analysis
Values are expressed as the mean±standard deviation. Univariate comparisons of continuous variables were conducted using the unpaired Student's t-test. Univariate analyses of the differences in proportion between the two groups were accomplished using a chi-square analysis. Differences with a p of <0.05 were considered statistically significant.
Results
Patient characteristics
Of the 260 total patients, there were 157 males and 103 females. The age of the patients on the time of symptom onset by tachycardia ranged from 1 to 17 years of age, with a mean of 12.30±3.06 years of age. The age of the patients on the time of RFCA ranged from 2 to 18 years of age, with a mean of 13.7±3.4 years of age. On the time of RFCA, 9 patients (3%) were younger than 6 years of age, 76 patients (30%) were between 7 and 12 years of age, and 175 patients (67%) were older than 12 years of age. EPS and RFCA for AVRT, atrioventricular nodal reentry tachycardia (AVNRT), ventricular tachycardia (VT) and atrial tachycardia (AT) as tachycardia mechanisms was performed on 13.2±3.5 years of age (range 2-18 years of age), 14.2±3.6 years of age (range 8-18 years of age), 16.0±1.9 years of age (range 13-18 years of age), and 17.5±0.7 years of age (range 17-18 years of age), respectively. In addition, RFCA was performed on an average of 13.7 pediatric patients per year.
Sixty-four patients (24.6%) required sedation using diazepam, ketamine, or propofol.
Three of the patients were less than 5 years of age, 2 patients were 2 years of age, and 1 patient was 3 years of age. All of them had CHD, and RFCA was performed due to recurrent SVT before surgery for CHD.
Tachycardia mechanisms
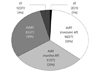
Tachycardia was seen 272 times in 260 patients.
The most frequent tachycardia mechanism was AVRT, which was observed in 175 patients.
AVNRT was observed in 83 patients. AVRT occurred more frequently than AVNRT (65% vs. 30%, p=0.0001). VT and AT were observed in 12 and 2 patients, respectively. The tachycardia mechanisms are summarized in Fig. 1.
Four patients (2%) had AVNRT and AVRT simultaneously. Among of them, the AVRT of 3 patients was induced by concealed AP and the AVRT of 1 patient was induced by manifest AP.
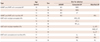
In nine patients, AVRT was induced by multiple APs. Of them, three patients had concealed and manifest APs simultaneously, 3 patients had two manifest APs, and 3 patients had two concealed APs. The characteristics of them are summarized in Table 1.
Atrioventricular reentry tachycardia
In patients with AVRT, a total of 175 APs, including multiple APs counted separately, was identified. The locations of APs were determined by the ablation site and are illustrated in Figs. 2 and 3.
Of 175 APs, 94 APs were concealed APs (Fig. 2), 79% of them (74/94) was located on the left. The most common site for left-side APs was the left lateral wall (43/74, 58%). On the other hand, 81 APs were manifest APs (Fig. 3), and 60% of them (49/81) was located on the right. The three most common sites of manifest APs were the left lateral wall (19/81, 23%), the right posteroseptal wall (12/81, 15%), and the right lateral wall (10/81, 12%). Left-side APs were more common in concealed APs than in manifest APs (74/94 vs. 32/81, p<0.001).
The success rate of RFCA for AVRT was 92% (161/175). After initial RFCA was done, 12 cases recurred; right- and left-side APs accounted for 50% (7/12) and 50% (7/12), respectively. In recurred cases, RFCA was repeated and was successful in all cases. Fourteen cases had failure of RFCA. Of the failed RFCA cases, there were 5 concealed APs and 9 manifest APs; right- and left-side APs accounted for 64% (9/14) and 36% (5/14), respectively. Five APs were located in the right anterior wall, 3 APs in the right posterior wall, 1 AP in the para-Hisian, 4 APs in the left anterior wall, and 1 AP in the left posterior wall.
Atrioventricular nodal reentry tachycardia
AVNRT was detected in 83 patients. Seventy-eight patients showed typical AVNRT and 5 patients showed atypical AVNRT. An ablation of the midseptal (M1 and/or M2) region was performed in 55 patients (66%). An ablation of the anteroseptal (A 1 or 2) region, which carried a high risk of atrioventricular (AV) node injury, was performed in 3 patients; 2 of these patients had intact AV node conduction afterwards.
The success rate of RFCA for AVNRT was 100% (83/83). Recurrence or failure of ablation was not observed in the patients with AVNRT.
Ventricular tachycardia and atrial tachycardia
VT originated in the mid-inferoseptum in 9 patients, the left ventricular outlet tract (LVOT) in 2 patients, and the right ventricular outlet tract in 1 patient.
The success rate of RFCA was 92% (11/12) for VT. After initial RFCA, VT induced from LV apex recurred in one patient. RFCA failed in 1 LVOT VT.
Two patients had intraatrial reentry tachycardia. A successful RFCA was performed in one patient but failed in the second patient.
Influence of age on tachycardia mechanism and accessory pathways location
In the time of RFCA, AVNRT patients were older than AVRT patients (14.2±2.6 years vs. 13.2±3.5 years, p=0.018). However, in the time of first symptom, there was no significant difference between AVNRT patients and AVRT patients (13.3±3.1 years vs.13.0±2.6 years, p=0.523). Although AVNRT occurred more commonly in older age than in younger age, there was no significant difference between tachycardia mechanism and age (Fig. 4). There were no statistical differences between properties of APs (concealed vs. manifest APs), and locations of APs (right vs. left APs) according to age.
Complications
Complete atrioventricular block (CAVB) developed in one patient with AVNRT. However, because she maintained an acceptable heart rate and exercise tolerance, a pacemaker was not implanted. Other procedure-related complications, such as valve dysfunction, myocardial perforation, and thromboembolic events, were not documented.
Combined cardiac disease
Associated cardiac disease was detected in 5 patients, including 2 functional univentricular hearts, 1 Ebstein's anomaly, 1 atrial septal defect and 1 mitral valve prolapse. All of these patients had AVRT and APs for AVRT were located on the left side in 3 patients and on the right side in 2 patients. One right-side AP was manifest AP and the others were concealed APs. Their characteristics are summarized in Table 2.
Discussion
From our long-term experience with RFCA in children and adolescents, we have the following main findings: 1) the most common tachycardia mechanism that required RFCA was AVRT, 2) 5% of the patients that had multiple tachycardia mechanism or APs, 3) concealed APs were located more on the left than right, while manifest APs were located on the right, and 4) the overall final success rate of RFCA was 95%.
In the present study, the most common tachycardia mechanism was AVRT, which accounted for 65%, and AVNRT, which accounted for 30%. Additionally, the AVNRT patients were older than AVRT patients. In one previous study with 131 pediatric patients ≤15 years old enrolled from 1992 to 2003, AVRT occurred in 70.4% of the patients (93 of 131 patients), AVNRT in 20.5% (27 of 131 patients), VT in 4.5% (6 of 131 patients) and AT in 4.5% (6 of 131 patients).4) In another study with 100 patients ≤19 years old enrolled during the period from 2000 to 2004, AVRT occurred in 66% of the patients (66 of 100 patients), AVNRT in 16% (16 of 100 patients), VT in 6% (6 of 100 patients) and AT in 8% (8 of 100 patients).5) These studies also found that the age of AVNRT patients was greater than AVRT patients.4)5)
In adults with SVT, AVNRT is the most common tachyarrhythmia.7-10) On the other hand, the presence of SVT, AVNRT in children and adolescents is less common.10)11) Although the natural history of AVNRT in pediatric patients is poorly understood, it may be related to maturational changes in the AVN.8)12-14) Previous studies have shown that the morphology of AVN changes with age. These studies suggested a gradual increase in fibrofatty tissue within the AVN and changes in the position of the AVN caused by gradual expansion of the muscular AV septum.15)
We detected differences in the location of APs between manifest APs and concealed APs. Seventy-nine percent of concealed APs were located on the left, the most common site being the left lateral wall. On the other hand, 60% of manifest APs were located on the right, and the most common site was the right lateral wall and septum. However, from the results of this study, we could not suggest the significant relation between AP location and age. Our previous study showed that right-side manifest APs occurred more frequently in patients <18 years old (68%, 21/31) than in patients ≥18 years old (38%, 65/170), and left-side manifest APs occurred more frequently in patients ≥18 years old (62%, 105/170) than in patients <18 years old (32%, 10/31).16) In contrast with our results, a previous study on pediatric patients demonstrated that AVRT was induced by right-side APs than left-side APs (56.9% vs. 43.1%, 52.1% vs. 47.8%).4) Another report showed that right- and left-side APs were found in nearly the same proportions in children with manifest APs.17) A study on elderly patients >60 years of age with manifest APs showed that left lateral APs were predominent.18)
Multiple tachycardia mechanisms or multiple APs were not common. In the present study, only 5% of patients had multiple tachycardia mechanism (AVNRT+AVRT) or multiple APs. In agreement with our results, multiple APs were reported to occur in 5-9% of patients in other pediatric studies.4)5) One report on RFCA for infants with SVT demonstrated the incidence of multiple APs to be only 1%.19)
In this study, the final success rate following repeated RFCA in recurrent cases was 95%. Only one procedure was complicated by persistent CAVB, and there were no other documented events related to the procedure. Many reports for pediatric RFCA have shown that the major complication rate was very low and that RFCA in the management of SVT in children was safe and effective, which is in agreement with our results.4)5)17)20)
Our study demonstrated that the recurrence rate was 5%, and 92% of these cases were AVRT. The previous reports had shown that the recurrence rate was between 5% and 13% for AVRT and between 7% and 8% for AVNRT.4)5)17)20) Although there was no difference in the recurrence rate for different AP locations in our study, a previous report showed that the most common locations of APs in recurrent cases were the right anteroseptal and right lateral positions.4) In general, due to the structure of the right side of the heart, it might be difficult to keep the tip of the ablation catheter on the annular portion during radiofrequency current application as firmly as during RFCA of left-side APs, and failure of RFCA could occur.
Study limitations
Because this study was performed retrospectively, the frequency of tachycardia mechanisms could be influenced by the patient selection. Most of patients had a structurally normal heart and we could not suggest the characteristics for tachycardia mechanism, APs, recurrence and failure of RFCA according to type of CHD.
In conclusion, as in other pediatric studies, our study demonstrated that pediatric RFCA provides a good success rate and an acceptable recurrence and complication rate. In addition, we suggest that the APs location may be associated with concealed or manifest property of APs.




 XML Download
XML Download