

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite advances in pharmacotherapeutic strategies, congestive heart failure (HF) is a chronic disease and a major public health concern because of its high morbidity and mortality.1) In advanced HF with severe systolic dysfunction {left ventricular ejection fraction (LVEF) ≤35%} with wide QRS interval (>120 ms), device therapies such as cardiac resynchronization therapy (CRT) have been shown to improve prognosis.2-4)
Evidence from several studies revealed that CRT significantly reduces mortality and all-cause hospitalizations in patients with advanced HF.5)6) The Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure study demonstrated that use of CRT was associated with a significant 20% decrease in mortality of advanced HF at 6 month follow-up.5-8) The Cardiac Resynchronization-Heart Failure trial showed a significant 36% decrease in the combined end point of all-cause mortality and HF hospitalizations with CRT.5)6)
Recent studies revealed that CRT is still underutilized in clinical practice with significant variations despite being recommended.9) To facilitate the consideration of CRT, we investigated prognostic factors in patients with advanced HF who were suitable candidates for CRT but were treated by conventional strategy. In addition, we developed a risk model to identify the patients who had poor prognosis. The validity of this model was tested in a separate group of patients.
Subjects and Methods
Study population
Between January 2007 and February 2009, 1345 patients with HF visited the tertiary referral hospital (Severance Cardiovascular Hospital, South Korea). Of these, 239 patients (18%) who had advanced HF {New York Heart Association (NYHA) functional class II-IV and LVEF ≤35%} with a wide QRS interval (>120 ms) were consecutively enrolled. Patients 1) who received device therapy or heart transplantation and 2) who had a malignancy were excluded from this study (Fig. 1). For the validation of a risk model, 66 patients were enrolled from a different affiliated institution (Kangnam Severance Hospital, South Korea) with the same inclusion and exclusion criteria (validation cohort) during the same period.
Echocardiography and electrocardiogram measurements
Echocardiography was performed on all patients at the index visit. A standard echocardiography was performed and the left ventricular end diastolic diameter (LVEDD), left arterial volume index, and early mitral inflow velocity to early diastolic mitral annular velocity (E/E') were measured. LVEF was measured by the Simpson method. All electrocardiograms were recorded at a 25 mm/s sweep speed, and QRS duration was measured by 2 experienced cardiologists from lead V2.
Clinical and biochemical data
Demographic variables, co-morbidities, and medications were collected at the index visit. Biochemical data included the following variables: serum hemoglobin (Hb), hematocrit (Hct), creatinine (SCr), sodium (Na), and total cholesterol. The rhythm and QRS interval on ECG were also obtained and analyzed.
Outcomes
In order to identify and evaluate risk factors associated with prognosis in advanced HF, we retrospectively reviewed the clinical course. The primary end point of the study was all-cause death during the follow-up period. We also investigated a composite endpoint of all-cause death and unplanned hospitalization due to major adverse cardiovascular event (MACE; worsening HF, acute coronary syndrome, and fatal arrhythmia).
Statistical analysis
Continuous variables were expressed as the mean and standard deviations. Baseline characteristics were compared by chi-square analysis for dichotomous variables and Student's t-test for continuous variables. Cox proportional hazard regression analysis was performed to evaluate the relationship between risk factors and outcomes. To develop a prognostic model, we assigned the risk factors identified by multivariate analysis weighted points based on β regression coefficient values. Survival curves were constructed according to the Kaplan-Meier method and comparisons of the survival rate between risk groups were compared using the log-rank test. The discriminative ability of our prediction model was evaluated by receiver-operating curve analysis (C statistic). P were all 2-sided and considered to be statistically significant at p<0.05. SAS (version 9.1.3, SAS Institute Inc., Cary, NC, USA) was used for all statistical analysis.
Results
Patient characteristics
The clinical characteristics and the use of various cardiac medications at the time of enrollment are presented in Table 1. Our subject group consisted of 239 patients (160 males) with a mean age of 67±11 years. The mean duration of the follow-up was 308±236 days. From this group, 56 (23%) patients died. The etiology of HF included 131 (55%) ischemic cases and 108 (45%) non-ischemic cases. There were 131 (55%) hypertensive and 94 (39%) diabetic patients, and 141 (59%) were chronic kidney disease (CKD) patients. 77 (32%) patients suffered from atrial fibrillation.
The mean LVEF was 25±7% and the mean QRS interval was 145±20 ms. All patients were being treated with diuretics (68%), aldosterone receptor blockers (39%), angiotensin converting enzyme inhibitors (10%), angiotensin II receptor blockers (32%), and digoxin (27%). Beta-blockers were taken by only 12 (5%) patients.
All-cause death
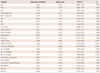
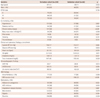
By the end of the study, all-cause death (primary end point) occurred in 56 (23%) patients. Table 2 presents the univariate analysis that identified risk factors affecting all-cause death. The following demographic, clinical, biochemical, and echocardiography variables had significant correlations with all-cause death: NYHA class (III, IV vs. II) {hazard ratio (HR) 4.2; 95% confidence interval (CI): 1.81 to 9.87; p<0.001}, body mass index (≥25 kg/m2) (1.7; 95% CI: 1.01 to 3.04; p=0.05), the presence of hypertension (0.5; 95% CI: 0.23 to 0.98; p=0.04), CKD (2.1; 95% CI: 1.17 to 3.75; p=0.01), prior stroke (2.1; 95% CI: 1.00 to 4.47; p=0.05), LVEF (≤25%) (2.7; 95% CI: 1.55 to 4.68; p<0.001), LVEDD (≥55 mm) (0.4; 95% CI: 0.21 to 0.65; p<0.001), heart rate (>90 bpm) (6.3; 95% CI: 3.7 to 10.6; p<0.001), serum Hb (2.7; 95% CI: 1.30 to 4.14; p<0.001), serum Na (≤135 mEq/L) (2.74; 95% CI: 1.62 to 4.63; p<0.001), and serum creatinine (≥1.5 mg/dL) (3.3; 95% CI: 1.96 to 5.69; p<0.001).
Next, we analyzed significant factors by stepwise multivariate analysis. Prior stroke (HR 2.7; 95% CI: 1.23 to 6.13; p=0.01), heart rate (>90 bpm) (4.6; 95% CI: 2.51 to 8.59; p<0.001), serum Na (≤135 mEq/L) (2.9; 95% CI: 1.61 to 5.37; p<0.001), and serum creatinine (≥1.5 mg/dL) (1.9; 95% CI: 1.02 to 3.64; p=0.04) were defined as significant predictors (Table 3).
All-cause death or unplanned hospitalization for a major cardiovascular event
The secondary end point (all-cause death or unplanned hospitalization due to MACE) occurred in 92 (38%) patients (Fig. 2). In multivariate analysis, NYHA class (III, IV vs. II) (2.0; 95% CI: 1.05 to 3.71; p=0.04), heart rate (>90 bpm) (2.16; 95% CI: 1.29 to 3.62; p=0.01), serum Na (<135 mEq/L) (2.53; 95% CI: 1.59 to 4.03; p<0.001), and serum creatinine (≥1.5 mg/dL) (2.1; 95% CI: 1.20 to 3.58; p=0.01) were identified as significant risk factors.
Prognostic modeling and risk stratification
We assigned scores to risk factors based on a linear transformation of the corresponding β regression coefficients, as previously described in Anis Rassi's article.10) The coefficient of each variable was divided by the lowest β value, then multiplied by a constant (2), and rounded to the nearest integer (Table 3).
The risk model calculated a score by adding together the points corresponding to patient's risk factors: {Risk score=3×prior stroke+5×heart rate (>90 bpm)+3×serum Na (≤135 mEq/L)+2×serum creatinine (≥1.5 mg/dL)}.
All patients were stratified into three groups based on risk score. The cut-points were obtained by maximizing the c-index: low-(0 point), intermediate-(1-5 points), and high-risk group (>5 points). There were 119 (50%) patients identified as low, 81 (34%) patients as intermediate and 39 patients identified (16%) as high-risk group.
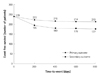
The 2-year mortality rates of each group were 5% (6/119), 31% (25/81), and 64% (25/39), respectively. Compared with the low-risk group, the HR of the high-risk group was 20.9 (95% CI: 8.6 to 51.3; p<0.001) and intermediate-risk group was 6.7 (95% CI: 2.7 to 16.3; p<0.001). The C statistic for the risk model for prediction of mortality was 0.78 (Fig. 3A, Table 4).
Atrial fibrillation and mortality
Although CRT in advanced HF with atrial fibrillation was not a class I indication,2) many studies have reported the benefits of CRT to advanced HF with atrial fibrillation.11) In our study, 77 patients had atrial fibrillation and 20 (26%) patients had died. We re-classified patients based on the risk score. In these patients, the high-risk group with atrial fibrillation showed higher mortality risk than the low-risk group (HR 32.1; 95% CI: 4.1-251.4; p=0.001).
Validation of the prediction model
A total of 66 patients from a different hospital were selected as the validation cohort (Table 1 and 5). During a mean follow-up of 686±367 days, 13 patients (20%) died. Classification of the validation cohort according to their risk score resulted in the assignment of 36 patients (55%) to the low-, 20 patients (30%) to the intermediate- and 10 patients (15%) to the high-risk groups. The 2-year mortality rates for these three groups were 3% (1/36), 30% (6/20), and 50% (5/10), respectively. The C statistic was 0.80. Compared with the low-risk group, the HR of the high-risk group was 12.9 (95% CI: 2.5 to 67.4; p=0.002) and intermediate-risk group was 6.2 (95% CI: 1.2 to 30.6; p=0.026) (Fig. 3B, Table 5).
Discussion
Our study demonstrated that patients with advanced HF who were suitable for CRT but treated with a conventional strategy exhibited high mortality (56 deaths, 23%) by the time of the follow-up examinations. The risk of death in advanced HF is predicted by the presence of 4 independent risk factors, which are prior stroke, heart rate (>90 bpm), serum Na (≤135 mEq/L), and serum creatinine (>1.5 mg/dL). We developed a risk model using these factors and stratified patients into the low-, intermediate-, and high-risk groups according to their risk score. The high-risk group demonstrated a 21-fold higher mortality risk compared to the low-risk group. This risk model was also validated in terms of risk stratification and mortality prediction.
Cardiac resynchronization therapy is a well-proven invasive device therapy in patients with advanced HF. It has been reported to improve ventricular conduction delay and ventricular function, reduce the magnitude of mitral regurgitation, and increase pulse pressure, cardiac index, as well as reverse remodeling of the ventricle.12) However, recent studies revealed that CRT is underutilized in clinical practice with significant variations associated with age, insurance, QRS interval, and geographic location of practices.9)13) An analysis from the Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting found that only 38.8% of patients who fit the guidelines for receiving CRT were implanted with a CRT device from May 2007 through June 2009 in the United States.13) Based on the European Medical Device Trade Organization registry, the number of CRT implantations markedly increased from 46/million in 2004 to 99/million in 2008. However, this rate (99/million) still indicated only 7% of all eligible HF patients received a CRT device.14)
To facilitate the use of CRT in eligible HF patients, effective risk stratification of advanced HF is crucial. Using our model, the high-risk group showed a markedly grave prognosis compared with the low-risk group (2-year mortality 64% vs. 5%, HR 20.9; 95% CI: 8.6 to 51.3; p<0.001).
Our prediction model is comprised of 4 independent risk variables. Stroke was proposed as an independent risk factor associated with poor prognosis in HF. This is because stroke is an indicator of severe LV dysfunction15) and shares common risk factors as well as pathophysiological mechanisms with coronary artery disease, which is the most common cause of HF.16)17) In the Enhanced Feedback for Effective Cardiac Treatment study, a stroke increased 30-day mortality (odds ratio 1.43; 95% CI: 1.22 to 2.27; p=0.03) among patients hospitalized for HF.8)
Tachycardia may be a sign of HF and play a role in the deterioration of cardiac pump function. Several types of tachycardia have been related to the development of HF, including atrial fibrillation/flutter, atrial tachycardia, atrioventricular nodal reentry tachycardia, and ventricular tachycardia.18)
Hyponatremia may also play a role in poor outcomes. This problem is largely related to the associated fall in cardiac output and systemic blood pressure. Patients with hyponatremia showed significantly increased mortality compared with normonatremic patients.19)
Many studies have reported that renal insufficiency is associated with adverse cardiovascular outcomes.20)21) McAlister et al.20) have shown that HF patients with renal insufficiency exhibited a 1% increase in mortality for each 1 mL/min decrease in creatinine clearance.20)
In our study, prolongation of the QRS interval and enlarged LVEDD were not independent predictors for mortality. There was no significant difference in QRS interval between the survivor and non-survivor groups. This finding is in disagreement with previous studies concerning the prognosis of HF, in which the prolongation of the QRS interval was generally associated with poor prognosis in HF.22) This discrepancy is possibly due to the prolonged QRS interval (>120 ms) in all enrolled patients.
Left ventricular end diastolic diameter is a known risk factor in the prognosis of patients with systolic dysfunction and HF.23) In our study, LVEDD was associated with lower odds of all-cause mortality based on univariate analysis. This disagreement with previous studies may be attributed to the enlarged (>55 mm) status of LVEDD in most of the enrolled patients. Even though mean LVEDD of survivor was slightly larger than the non-survivor, the proportion of patients with severe LV dilatation (LVEDD ≥75 mm) was higher in the non-survivor group (16.1% vs. 13.1%).
Regarding survival in severe HF, we already have several models for evaluation. The Seattle Heart Failure model suggests a 3-year survival rate in HF and the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness risk model predicts 6 month mortality for acute decompensated HF patients.24)25)
These two prediction models are more accurate predictors of survival of advanced HF patients than our prediction model. However, these scoring models require more than 10 variables and invasive procedures like pulmonary catheterization for accurate prediction. In contrast, our prediction model consists of only four risk factors and does not require any invasive procedure.
Our study has several limitations. First, we did not exclude atrial fibrillation patients. Even though advanced HF with atrial fibrillation is not a class I indication for CRT, many studies reported that these patients also benefit from CRT. In a meta-analysis of prospective cohort studies,11) patients in atrial fibrillation had similar improvement in LVEF with no significant mortality difference compared to patients with a normal sinus rhythm. In our study, patients with atrial fibrillation were effectively stratified into risk groups using a risk model. The high-risk group demonstrated a 32-fold higher mortality than the low-risk group.
Second, as it was a retrospective design study, our results are dependent on the accuracy of medical records. Therefore the accuracy of our decision about optimal cardiac medication is lacking. Additionally, we enrolled patients from tertiary referral hospitals and had a relatively small validation cohort, which may not fully represent the entire spectrum of advanced HF.
In conclusion, the prognosis of patients suffering from advanced HF with low LVEF and a wide QRS interval who were treated with a conventional strategy is primarily dependent on prior stroke, heart rate, serum Na, and serum creatinine. We developed a risk model based on these four factors that predict mortality risk and stratified patients into three levels of risk (low, intermediate, and high) effectively. This model may be useful to clinicians for predicting the patient's prognosis, and CRT should be actively considered in high-risk patients.





 XML Download
XML Download