

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hyperkalemia is a common side-effect of heart failure treatment. The prevalence of hyperkalemia in the general population is unknown but reported to be 1-10% in hospitalized patients.1-4) The most common predisposing factors are impaired kidney function and drugs such as angiotensin-converting enzyme inhibitors, angiotensin-II receptor antagonists, and aldosterone antagonists.1)5)6) Cardiac manifestations of hyperkalemia are sometimes lethal with various presentations. The common electrocardiographic changes in patients with hyperkalemia include a tented T wave, PR interval prolongation, QRS widening, ventricular fibrillation, and asystole. It has been suggested that hyperkalemia may be associated with transient sinus conversion of atrial fibrillation (AF), and, indeed, we report here a case of hyperkalemia resulting in sinus conversion from permanent AF.
Case
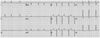
A 74-year-old woman was admitted to the hospital for diarrhea and epigastric pain. She had a history of hypertension, diabetes mellitus, chronic kidney disease, dilated cardiomyopathy, and permanent AF for 5 years (Fig. 1). Echocardiography performed 3 months before admission revealed severe global left ventricular hypokinesia (ejection fraction=19% by Simpson's method) and an enlarged left atrium (left atrial volume index=40 mL/m2). Her medications included digoxin (0.125 mg daily), warfarin (2 mg daily), ramipril (10 mg daily), furosemide (40 mg daily), spinolactone (25 mg daily), and carvedilol (25 mg daily).
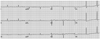
On examination, her heart rate was 41 bpm, and blood pressure was 110/70 mm Hg. Heart sounds were regular, and there were no murmurs or thrills. An electrocardiogram (ECG) revealed junctional rhythm at a rate of 35 bpm and a QRS duration of 136 msec (Fig. 2). Admission laboratory results showed severe hyperkalemia (serum potassium 8.3 mEq/L), high blood urea nitrogen (62.4 mg/dL), creatinine of 4.0 mg/dL, glucose of 248 mg/dL, and low sodium (131 mM) and hemoglobin (7.2 g/dL) levels. Arterial blood gas analysis on room air showed a pH of 7.400, pCO2 of 41.6 mm Hg, pO2 of 102.8 mm Hg, and HCO3- of 26.0 mmol/L.
The patient was immediately treated with intravenous calcium chloride, followed by intravenous glucose/insulin and a sodium bicarbonate infusion. On hospital day 2, the serum potassium level was 5.3 mEq/L and the ECG showed sinus bradycardia at a rate of 53 bpm with an 80 ms QRS duration (Fig. 3). On hospital day 3, the ECG revealed a normal sinus rhythm at a rate of 67 bpm, and the serum potassium level was within normal limits (4.3 mEq/L). The patient was discharged 6 days after admission, and the ECG at discharge showed normal sinus rhythm at a rate of 65 bpm with occasional premature ventricular complexes. At the 10 day and 1 month follow-ups, the ECG at an outpatient clinic had returned to AF and serum potassium levels were within the normal range.
Discussion
Hyperkalemia causes various ECG changes. In mild to moderate hyperkalemia, depression of conduction between cardiac myocytes results in prolongation of the PR and QRS intervals as potassium levels increase. Severe hyperkalemia induces suppression of sinoatrial and atrioventricular conduction, resulting in sinoatrial and atrioventricular blocks, escape beats, and escape rhythms.7) At extremely high serum potassium levels, the QRS complex is markedly widened and fused with the T wave, creating a sine-wave appearance on ECG.8)
Interestingly, previous reports have documented unusual cardiac manifestations related to hyperkalemia, including pacemaker capture and sensing failure,9)10) loss of the delta wave in patients with Wolff-Parkinson-White syndrome,7) and transient sinus conversion of permanent AF during treatment for hyperkalemia.11-13) However, the mechanisms in these cases were not clearly defined.
In this case, the ECG on admission showed junctional bradycardia with a widened QRS complex. The ECG recovered to sinus bradycardia after the shift of potassium from the intracellular to extracellular space induced by intravenous glucose/insulin and sodium bicarbonate. Transmembrane permeabililty increases with the development of hyperkalemia and causes potassium influx into cells,5) which, in turn, causes decreased and shortened cellular action potentials by inactivating the sodium channel5)8)14) and delayed conduction between myocytes. As a result, hyperkalemia decreases excitability of atrial tissue, suppressing an irritable atrial ectopic focus and reentrant circuit.11) The ECG findings of junctional bradycardia with widening of the QRS complex on admission are explained by these mechanisms. Because the sinus node is less sensitive to high potassium level than atrial tissue, hyperkalemia suppresses sinus nodal function to a lesser degree than atrial tissue conduction.11) Therefore, sinus rhythm may recover earlier than AF activity in patients with permanent AF during treatment for hyperkalemia.
The latter phenomena have some similarities with pharmacological characteristics of amiodarone, which is the most effective antiarrhythmic drug available for maintaining sinus rhythm in patients with AF. Oral amiodarone results in pharmacological cardioversion of AF in up to 40% of patients.15) Amiodarone blocks potassium channels and inactivates sodium channels, thereby prolonging repolarization, action potential duration, and refractory period.16-19) Because the relative potency of these effects is greater in the atrium,20) amiodarone suppresses atrial ectopic activity and maintains sinus rhythm. During treatment for hyperkalemia, intracellular potassium depletion that occurs by the extracellular shift in potassium prolongs repolarization, action potential duration, and refractory period. These mechanisms are similar to amiodarone-induced sinus conversion by blocking the inward potassium channel.
The maintenance duration of sinus rhythm that occurs during treatment for hyperkalemia remains undetermined and appears to vary according to clinical course. In a case report of hyperkalemia-induced sinus conversion, sinus rhythm was maintained for 3 months after normalization of serum potassium level11) and another case report of permanent AF with severe hyperkalemia described transient sinus conversion of only 16 minutes duration.12) In our patient, the ECG returned to AF after 10 days of normal serum potassium levels. Therefore, sinus rhythm during the recovery phase of hyperkalemia seems to eventually revert to AF within several weeks to months, so it is necessary to maintain proper treatment for AF.
In conclusion, other than well-known ECG features of hyperkalemia, restoration of sinus rhythm in patients with AF may occur during treatment for hyperkalemia, so it is important to maintain treatment for AF even after sinus conversion.

 XML Download
XML Download