

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Oxidative stress is defined as the overproduction of reactive oxygen species (ROS) and free radicals beyond the physiological ability to detoxify or to repair. The considerable reactive properties of ROS cause oxidative damage to lipids, deoxyribonucleic acid (DNA), and proteins. Recent evidence suggests that ROS could have a role in the development of hypertension, dyslipidemia, diabetes mellitus (DM), and atherosclerosis.1)2) However, the specific parts played by oxidative processes remain the subject of active investigation.
Oxidative damage to lipids and DNA could serve as a useful biomarker to allow assessment of atherosclerotic cardiovascular disease. This could help to define atherosclerotic mechanisms and measurement of circulating levels of specific oxidant products that could improve the assessment of cardiovascular risk.
The prostaglandin, 8-iso-prostaglandin F2α (8-iso-PGF2α), is an isoprostane that is produced by the non-enzymatic peroxidation of arachidonic acid in membrane phospholipids.3) Measurement of 8-iso-PGF2α is a reliable tool for the identification of subjects with enhanced rates of lipid peroxidation. Enhanced formation of 8-iso-PGF2α has been reported in association with several cardiovascular risk factors, as well as atherosclerosis.4)5)
Deoxyguanosine is one of the constituents of DNA. When it is oxidized, it is converted to 8-hydroxydeoxyguanine (8-OHdG). The compound, 8-OHdG, is the most frequently detected and studied that is the result of DNA lesions. A body of evidence indicates that urinary 8-OHdG is a biomarker of generalized cellular oxidative stress and may be a risk factor for cancer, atherosclerosis, and DM.6)
Data focusing on the clinical application and comparison of the oxidation products of lipid peroxidation (8-iso-PGF2α) or DNA damage (8-OHdG) in patients with stable coronary artery disease (CAD) are lacking. Therefore, we studied the associations of urinary 8-iso-PGF2α or 8-OHdG with stable angina and significant CAD.
Subjects and Methods
Study subjects
On a prospective basis, we enrolled 104 consecutive stable angina pectoris patients (ratio of cases : controls=1 : 2) with ischemia or equivocal on noninvasive testing who had undergone coronary angiography at Wonju Christian Hospital. We compared the CAD group with the non-CAD group. The CAD group (n=35) was defined as subjects with stable angina plus significant CAD according to coronary angiography. Significant CAD was diagnosed by the visual assessment of ≥70% luminal narrowing in any of the 3 major coronary arteries or ≥50% luminal narrowing of the left main coronary artery. The non-CAD group (n=69) was defined as patients with stable angina and atypical chest pain plus minimal CAD (<50% luminal narrowing in any of the 3 major coronary arteries) or normal-looking arteries according to coronary angiography. Subjects were excluded if they had evidence of heart failure, renal failure, infectious disease, or acute coronary syndrome. All subjects provided their informed consent, and the study protocol was approved by the Institutional Review Board of Wonju Christian Hospital.
Laboratory measurements of oxidative products
The first urine sample was drawn from each subject after fasting for 12 hours or overnight. Samples were separated immediately after collection by centrifugation at 3000 rpm for 10 minutes and stored at -80℃ until analyses. The supernatant was used for the determination of 8-OHdG (OXIS International Inc., Beverly Hills, CA, USA) and 8-iso-PGF2α (Stressgen Biotechnologies Inc., San Diego, CA, USA) with a competitive enzyme-linked immunosorbent assay (ELISA). The intra-assay coefficient of variation was 5.1% for 8-OHdG and 5.8% for 8-iso-PGF2α. The urinary 8-OHdG: creatinine and 8-iso-PGF2α: creatinine ratios were used in the analysis.
Statistical analyses
Data are expressed as frequencies, means, and median values (low quartiles and high quartiles). Distributions of continuous variables were examined for skewness and kurtosis and were logarithmically transformed (if appropriate). We used the Student's t-test, Mann-Whitney U test, or chi-square test to compare the differences between case and control groups.
Multivariable logistic regression was used to assess the independent associations between tertiles or continuous increments in the levels of 8-OHdG and 8-iso-PGF2α and significant CAD. We used 2 models with degrees of adjustment. First, we undertook an age- and sex-adjusted analysis (model A). Second, we further adjusted for hypertension (yes/no), DM (yes/no), body mass index (continuous variable), smoking (current/former/never), high-sensitivity C-reactive protein (continuous variable), low density lipoprotein-cholesterol (LDL-C; continuous variable), high density lipoprotein-cholesterol (HDL-C; continuous variable) and triglyceride (continuous variable) (model B).
Results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was determined at p<0.05 for all comparisons. All analyses were done using a Windows-based Statistical Package for the Social Sciences statistical package (version 12.0; SPSS Inc., Chicago, IL, USA).
Results
The prevalence of history of hypertension was significantly higher and HDL-C level was significantly lower in patients who CAD compared with non-CAD subjects. Median levels of 8-iso-PGF2α were significantly higher in the CAD group compared with the non-CAD group (9.2 vs. 6.0 ng/mg, p=0.001). There were no significant differences in 8-OHdG values between the 2 groups (Table 1).
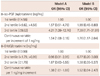
In the age- and sex-adjusted model (model A), ORs for CAD comparing tertiles 2 and 3 vs. tertile 1 of 8-iso-PGF2α were 1.57 (95% CI, 0.51-4.79) and 4.21 (95% CI, 1.39-12.76), respectively. After adjustment for multiple risk factors (model B), the OR for CAD in the highest tertile compared with the lowest tertile was 7.39 (95% CI, 1.71-31.91). When the 8-iso-PGF2α level was introduced as a continuous variable, the OR for CAD associated with an increase of 1 ng/mg in 8-iso-PGF2α level was 1.54 (95% CI, 1.08-2.18) in model A and 1.76 (95% CI, 1.17-2.64) in model B. The OR for CAD for the 8-OHdG level (continuous variable) was 1.38 (95% CI, 1.01-1.88) in model A. However, other ORs for the 8-OHdG level were not significant in models A and B (Table 2).
There was no significant difference in the median values of 8-iso-PGF2α between single- and multi-vessel disease (9.5 vs. 12.5 ng/mg, p=0.678).
Discussion
In this case-control study, we found that significant CAD was associated with the urinary 8-iso-PGF2α level, a surrogate of lipid peroxidation. However, 8-OHdG as an DNA oxidation product was not associated with CAD.
Lipid peroxidation has been considered to be a key mechanism for the development of atherosclerosis and inflammatory damage to blood vessels. Oxidation of LDL-C makes them susceptible to uptake by macrophages. This incorporation and accumulation into macrophages is a major cause of transformation of foam cells, vascular inflammation, and plaque formation.7)8) The compound, 8-iso-PGF2α, is formed by a non-enzymatic attack by free radicals on arachidonic acid (a component of lipid cell membranes). Studies have shown that urinary 8-iso-PGF2α may be the most reliable marker to assess lipid peroxidation in chronic disease.9-11) Increased levels of 8-iso-PGF2α are associated with aging, hypertension, DM, hypercholestolemia, smoking, and CAD.4)5)12) In the present study, we found that urinary levels of 8-iso-PGF2α using ELISA were associated with significant CAD compared with those of minimal CAD and normal CAD after adjustment for the important risk factors of CAD. This finding supports the concept that there might be a relationship between urinary concentrations of 8-iso-PGF2α and the severity of CAD. However, we failed to demonstrate a difference between single- and multi-vessel CAD. Further studies will be needed to find the association between 8-iso-PGF2α concentrations and the severity of atherosclerosis.
Deoxyribonucleic acid damage induces apoptosis in atherosclerotic plaques if DNA damage cannot be repaired by physiological mechanisms. Endothelial apoptosis is an early event in atherogenesis and triggers plaque formation.13) Apoptosis of vascular smooth muscle cells is associated with the growth and rupture of plaque due to the inflammation and remodeling of blood vessels.14)15) Therefore, oxidative DNA damage may have a role in the pathogenesis of atherosclerosis.
The compound, 8-OHdG, is an oxidized nucleoside of DNA. It is a valid marker for measuring the DNA damage caused by oxidative stress.6) Elevated levels of 8-OHdG are related with various states of malignancy,16) DM,17) peripheral arterial disease,18) and heart failure.19) However, there were no significant differences between the CAD and non-CAD group in the present study with respect to this parameter. These results suggest that lipid peroxidation is more important than oxidative damage to DNA in patients with CAD.
Two limitations must be considered when interpreting the results of the present. First, this study was of a case-control design from which cause-effect relationships could not be concluded. Second, these results cannot be generalized to all patients with CAD, because the study population was relatively small and because we excluded patients with unstable CAD.

 XML Download
XML Download