

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
High on-treatment platelet reactivity (HOPR) to antiplatelet therapy has been shown to be associated with atherothrombotic cardiovascular complications after percutaneous coronary intervention (PCI).1-3) Small dense low density lipoproteins (sd-LDL) have become recognized as a potential risk factor of coronary and noncoronary forms of atherosclerosis.4)7) They penetrate the arterial wall more easily and have high binding affinity to arterial proteoglycan, resulting in subendothelial accumulation in the early stage of atherogenesis.8)9) Furthermore, sd-LDL particles may enhance thromboxane synthesis and promote platelet aggregation.10) If sd-LDL is associated with HOPR in patients, this may suggest therapeutic implication of a more intensive treatment of dyslipidemia. Thus, we aimed to examine the possible relationship between LDL particle size and on-treatment platelet reactivity (OPR) in patients receiving antiplatelet therapy.
Subjects and Methods
Subjects
The LOw density LIPOprotein-cholesterol Particle Size measurement study was a prospective registry that included patients with coronary artery disease who had undergone a lipid profile analysis and measurement of LDL particle size at Seoul National University and Bundang Hospital. The inclusion criteria for the present analysis were patients who had undergone PCI and received dual antiplatelet therapy with aspirin and clopidogrel. From January 2009 through March 2010, a total of 434 consecutive patients were enrolled and all patients underwent platelet function testing. Patients with the following conditions were excluded from the study: on longterm (more than 2 weeks) statin therapy before lipid particle size measurement, with chronic renal failure, had severe hepatic failure, or had a cancer malignancy.
The diagnosis of diabetes mellitus was based on a history of treatment with either oral anti-diabetic agents or insulin or HbA1c ≥6.5%. Hypertension was defined as a history of treatment with anti-hypertensive agents or systolic blood pressure >140 mm Hg or diastolic blood pressure >90 mm Hg. Body mass index was calculated as weight (kg)/height2 (m2).
Lipoprotein and low density lipoprotein particle size measurement
Fasting blood samples were obtained by venipuncture on the day of the PCI. Serum was separated by centrifugation and biochemical measurements were conducted immediately. Serum glucose, total cholesterol (TC), low density lipoprotein-cholesterol (LDL-C), high density lipoprotein-cholesterol (HDL-C), and triglyceride were measured enzymatically using the Hitachi 747 chemical analyzer (Hitachi, Tokyo, Japan).
Low density lipoprotein particle size was determined using a gel electrophoresis (Lipoprint™ System; Quantimetrix Corp., Redondo Beach, CA, USA) according to the manufacturer's instructions.11) This method estimates LDL particle size by comparing their electrophoretic mobility using very low density lipoprotein as the starting point {Retention factor (Rf)=0} and HDL-as the end point (Rf=1). Because the Rf value obtained by this method correlated well with the peak LDL size obtained by ultracentrifugation,12) LDL peak particle sizes (PPS) could be derived from the work of Kazumi et al.13) {PPS=(1.429-Rf)×25} and the PPS values of the LDL-1 to LDL-7 bands were 27.7, 26.1, 24.5, 23.0, 21.8, 20.7 and 18.7 nm, respectively.14) The mean LDL particle diameter (in nm) was expressed as the weighted average of the PPS of all LDL subfractions as follows: Σ(LDLi/ΣLDLi)×sizei. LDLi was the area of the LDL bands relative to LDL-C and sizei was the PPS of the LDL band. We categorized patients into pattern A (large, buoyant LDL dominant) and pattern B (small, dense LDL dominant) by mean LDL particle diameter and cutoff value was defined as the smallest quartile (26.5 nm).15) Mean particle diameter over 26.5 nm was defined as pattern A and diameter of ≤26.5 nm was defined as pattern B. The sd-LDL fraction (%) was measured as proportion of sd-LDL (sum of subtypes LDL3-LDL7) to the sum of LDL1-LDL7.
Platelet function test
The magnitude of OPR was quantified using the VerifyNow™ system (Accumetrics, Inc., San Diego, CA, USA). The VerifyNow™ system is a whole blood cartridge-based method to determine the magnitude of platelet agglutination induced by either arachidonic acid in the aspirin assay and adenosine diphosphate (ADP) and prostaglandin E1 in P2Y12 assay.16) Platelet reactivity was reported as aspirin reaction units (ARU) and P2Y12 reaction units (PRU) and higher reaction unit reflected higher OPR. HOPR was defined as OPR greater than 454 ARU2) or 264 PRU17) according to previous studies. OPR was measured on the morning after drug administration in chronic users and 12-24 hours after loading dose (300 mg for aspirin, and 300-600 mg of clopidogrel) for naïve patients.
Statistical analysis
Continuous variables were presented as either mean±SDs or median with interquartile ranges and categorical variables as numbers and percentages. A comparison of continuous variables was performed using the Student's t-test or in case of non-normal distribution, Mann-Whitney U test when appropriate. Categorical variables were compared using chi-square test or Fisher's test when appropriate. Pearson's correlation coefficient was used to assess association between LDL particle size and OPR. Univariate and multivariate logistic regression analyses were performed to adjust for possible confounding effects of clinical characteristics and laboratory findings on the occurrence of HOPR.
Statistical Package for the Social Sciences Statistics (IBM Corporation, NY, USA) version 19.0 was used for all statistical analyses and p<0.05 was considered statistically significant.
Results
Population characteristics
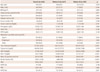
The clinical characteristics of the 434 patients included in the analysis were shown in Table 1 according to the pattern of LDL particle size. The mean LDL particle size of the patients was 26.74±0.56 nm (median 26.8 nm, inter-quartile range 26.5-27.1 nm) included in this study. Patients with pattern B were less likely to have been treated with statins before admission {153 (46.8%) vs. 36 (33.6%), p=0.019}, leading to higher TC (146.13±34.71 vs. 169.10±35.31 mg/dL, p<0.001) and lower HDL (35.69±10.06 vs. 31.15±7.47 mg/dL, p<0.001) in these patients.
Otherwise, there were no significant differences in clinical characteristics between pattern A and B. In addition, the mean ARU and PRU as well as the frequency of high on-aspirin platelet reactivity (HAPR, ARU>454) and high on-clopidogrel platelet reactivity (HCPR, PRU>264) were not different between the 2 groups. Statin medication before admission was the only significant predictor of pattern B on univariate and multivariate analyses.
Relationship between mean low density lipoprotein particle size and platelet reactivity
There was no significant correlation between mean LDL particle size and ARU level (r=0.080, p=0.098). Similarly, PRU levels were not correlated with mean LDL particle size (r=-0.027, p=0.568) (Fig. 1). Also in non-acute coronary syndrome (ACS) patients, there were no significant correlations among mean LDL particle size and ARU (r=-0.015, p=0.826) or PRU (r=-0.125, p=0.076) levels.
Clinical characteristics of patients with high on-aspirin platelet reactivity
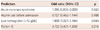
Next, patients were grouped according to whether they had HAPR or HCPR. A total of 148 patients was identified as having HAPR (Table 2). Compared with the non-HAPR group, those in the HAPR group were older (63.5±9.3 vs. 65.8±10.5 years, p=0.023), had lower hemoglobin (13.60±1.73 vs. 12.92±1.63 mg/dL, p<0.001), slightly higher serum creatinine (1.09±0.30 vs. 1.20±0.68 mg/dL, p=0.065) and HbA1c (6.67±1.12 vs. 7.00±1.50%, p=0.065). The differences in mean LDL particle diameter between the 2 groups were not statistically significant (26.70±0.57 vs. 26.80±0.55 nm in non-HAPR vs. HAPR group, p=0.078). Even after adjustment for various differences, low serum hemoglobin {odds ratio (OR) 1.808, 95% confidence interval (CI) 1.027-3.184, p=0.040} was a significant predictor of HAPR, while pattern B was not (OR 0.722, 95% CI 0.431-1.209, p=0.216) (Table 3).
Clinical characteristics of patients with high on-clopidogrel platelet reactivity
A total of 181 patients were identified as having HCPR (Table 4). Patients in the HCPR group were also older (62.87±10.04 vs. 66.35±8.94 years, p<0.001), more likely to be diabetic (30.4% vs. 40.3%, p=0.04), hypertensive (61.7% vs. 71.8%, p=0.03), and less likely to be males (80.6% vs. 56.4%, p<0.001), or smokers (26.8% vs. 16.1%, p<0.001). Mean hemoglobin was significantly lower in the HCPR group (13.80±1.73 vs. 12.74±1.51 mg/dL, p<0.001). There were no differences in mean LDL particle diameters between the 2 groups (26.7±0.6 vs. 26.8±0.5 nm, p=0.857) and on multivariate analysis, pattern B was not a predictor of HCPR (OR 0.858, 95% CI 0.513-1.435, p=0.559). Low serum hemoglobin (OR 2.511, 95% CI 1.403-4.493, p=0.002) was a strong predictor of HCPR, while smoking showed a mild trend toward being protective against HCPR (OR 0.626, 95% CI 0.377-1.038, p=0.070) (Table 5).
Discussion
Appropriate antiplatelet response to anti-platelet therapy is important in patients with coronary artery disease and inter-individual differences in response to aspirin and clopidogrel have been previously reported. To the best of our knowledge, no previous study has addressed the relationship between LDL particle size and OPR. Thus, we analyzed whether LDL particle size was associated with both response to aspirin and clopidogrel in those with coronary artery disease. The major finding of this study was that LDL particle size was not significantly associated with OPR and was not an independent predictor of HOPR.
Theoretically, there are various pathways by which sd-LDL could possibly stimulate platelet reactivity. It may promote the thromboxane synthesis and further influence platelet aggregation.10) In addition, sd-LDL particles are more susceptible to oxidation than large LDL18) and oxidized LDL stimulates platelet function more effectively by diminishing nitric oxide (NO) synthase expression,19)20) blocking CD36 and scavenger receptor A.21) Thus, pattern B could be expected to enhance OPR. However, in the present study, there was no significant association between LDL particle size and platelet reactivity in vivo.
Besides the obvious conclusion that LDL particle size has no effect on platelet function, there may be other possible explanations for our findings. First, several pathways are involved in platelet function homeostasis, including thromboxane, ADP, thrombin, and NO. Although sd-LDL could promote thromboxane synthesis, this may not be enough to significantly alter platelet reactivity. Second, the number of patients analyzed in the study was modest at best, and therefore, the number of patients in the present study may not have been enough to confirm the small effect of sd-LDL on platelet function. Third, since we measured platelet function in patients on dual anti-platelet therapy, the effects of sd-LDL on platelet function could have been attenuated. We could at least confirm that the effect of sd-LDL did not significantly alter response to clopidogrel or aspirin. Further studies in a larger patient population who are naïve for anti-platelet agents using various platelet function assays will be required to confirm the true effect of sd-LDL on platelet function.
In the present analysis, lower serum hemoglobin was a strong predictor of both HAPR and HCPR. Previous studies suggested similar results. Lee et al.22) and Cecchi et al.23) reported that lower hematocrit was associated with HAPR and HCPR. Decreased erythrocyte mass could be associated with a low availability of NO, which inhibits platelet aggregation by increase of intracellular cyclic guanosine monophosphate levels in platelets.24) Also, erythrocytes were able to release ADP, which enhances NO release by platelets.25)
Cigarette smoking showed a mild trend toward being protective against HCPR. Many studies already reported enhanced clopidogrel response in smokers, so called "smokers' paradox". We recently reported that this phenomenon was dependent on cytochrome P4501A2 status, suggesting that the cytochrome P450 system may be involved in the mechanism of smokers' paradox.26)
In this study, mean LDL particle size of the patients was 26.74±0.56 nm and 25% of patients showed pattern B lipid profile. In the study of Kwon et al.15) of Korean population underwent coronary angiography, mean LDL size was 26.56 nm and 37.7% of patients were pattern B. Compared with other studies, our study showed larger mean LDL particle size and less proportion of pattern B patients. We presume that more than 40% of patients with statin premedication before admission contributed to this better lipid profile.
This study has several limitations. First, this was a cross-sectional analysis, and it is well known that results of platelet function tests can change over time. To completely explain the association between LDL particle size and platelet reactivity, recurrent measurement in the same person after treatment intervention of dyslipidemia is needed. Second, the time point of blood sampling was not exactly the same for all patients. Blood samples for LDL particle size was done at admission, while those for platelet function measurement were obtained 12-24 hours after loading dose of aspirin and clopidogrel for naïve patients. In addition, about half of the study population had ACS. Since it is widely known that serum TC and LDL-C levels decrease early after ACS,27)28) LDL particle size also could be altered after ACS and that could be a confounding factor. So all the multivariate analyses were adjusted for the diagnosis of ACS and showed that ACS was not a significant predictor of pattern B, HAPR, and HCPR. Furthermore, additional analysis for only non-ACS population presented a lack of association between LDL particle size and OPR.
Although sd-LDL is emerging as a potential risk factor of atherosclerosis, the atherogenic mechanism of sd-LDL is poorly understood. Further studies about atherogenic and thrombogenic potential of sd-LDL may be needed to evaluate clinical implication of sd-LDL in patients with coronary artery disease.
In conclusion, there was no significant association between LDL particle size and OPR in patients with coronary artery disease.




 XML Download
XML Download