

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Congenital coronary anomalies are present in approximately 1% of patients referred for cardiac catheterization.1-3) However, the incidence was found to be 5.6% in a recent prospective angiographic study of 1950 consecutive cases.4) Among these, an anomalous origin of right coronary artery (RCA) from the left sinus was found in approximately 0.03-0.09% of patients undergoing coronary angiography (CAG).5) An anomalous origin of RCA from the ascending aorta above the left sinus of valsalva is associated with angina pectoris, acute myocardial infarction or sudden cardiac arrest when it courses between the aorta and the pulmonary trunk.6)7) Additionally, a case of sinus of valsalva aneurysms with ventricular septal defect is an extremely rare cardiac anomaly that may be acquired or congenital. We report here a case of successful percutaneous coronary intervention (PCI) by using multidetector computed tomography (MDCT) and intravascular ultrasound (IVUS) in a patient who had an anomalous RCA arising from the ascending aorta with a history of open heart surgery due to ruptured sinus of valsalva and ventricular septal defect, including a review of the relevant literature.
Case
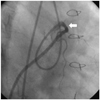
A 39-year-old man was admitted to the emergency room with accelerating effort chest pain for four months. The patient had past history in which patch closure was performed for rupture of sinus of valsalva and ventricular septal defect twenty years ago. The operator could not find the RCA which was at the presumed site according to the operation record. The physical examination showed normal findings. The results of complete blood count, blood chemistry, and urinalysis were normal. The electrocardiogram showed sinus bradycardia and left ventricular hypertrophy. Chest radiography revealed borderline cardiomegaly with mild congestion of the pulmonary vasculature. Transthoracic echocardiography showed akinesia of basal septum and mid to basal inferior wall with mild left ventricular systolic dysfunction (ejection fraction=51%). He was sus-pected of RCA ischemia and referred to the cardiac catheterization laboratory for CAG. In addition, the left coronary angiogram was normal (Fig. 1C). However, we could not easily engage the RCA using several catheters such as 6 French (Fr) sized jukdin 3.5 & 4.0 and amplatz left 1 & 2 (Cordis Corporation, Miami, FL, USA). Therefore, we decided to perform an aortogram, which showed the anomalous position of the RCA ostium originating from the tubular portion of the ascending aorta above the left coronary cusp (Fig. 1A and B). We decided to delay the PCI and took MDCT CAG images for obtaining information about precise coronary anatomy. The MDCT CAG images revealed an anomalous origin of RCA from the tubular portion of the ascending aorta with acute angulation and subsequent slit-like luminal narrowing of the proximal RCA between the pulmonary trunk and ascending aorta (Fig. 2). The next day, we tried CAG again and successfully engaged the RCA using 6 Fr Launcher extra-backup 4.5 guiding catheter (Medtronic, Inc., Minneapolis, MN, USA) via a transfemoral approach. The RCA showed a subtotal occlusion in its proximal portion (Fig. 3). We inserted a ChoICE™ PT guide wire (Boston Scientific, Heredia, Costa Rica) into RCA and dilated the lesion using a 3.0×20 mm sized VOYAGER balloon (Abott Vascular, Santa Clara, CA, USA) at 12 atmosphere. Next, an IVUS study was performed, which study showed atherosclerotic plaque burden on the proximal RCA with a spindle shaped arterial lumen (a slit-like lumen) caused by extrinsic compression (Fig. 4A). We implanted a 3.0×38 mm sized Endeavor Resolute stent (Medtronic, Galway, Ireland) at 12 atmosphere and dilated the stent using a 3.0×12 mm sized Quantum balloon (Boston Scietific, Maple Grove, MN, USA) at 20 atmosphere. The IVUS study then showed a successfully implanted stent at the proximal RCA (Fig. 4B). The final angiogram showed successful revascularization of the RCA (Fig. 5). We finished the procedure without any peri-procedural complications. His symptoms subsided and he was discharged the next day. The patient is still doing well a year after the PCI.
Discussion
Sinus of valsalva aneurysms are very uncommon, with an incidence ranging from 0.1% to 3.5% of all congenital heart defects.8) Sinus of valsalva aneurysms have a marked male preponderance (4 : 1), and their incidence is the highest in Asian populations. Most sinus of valsalva aneurysms arise from the right or non-coronary sinuses, and commonly protrude and rupture into the right ventricle or right atrium. Aneurysms may also rupture into the left ventricle, pulmonary artery, left artrium, or pericardial cavity.8)9) The combination of a sinus of valsava aneurysm and anomalous origin of coronary artery is quite rare, but should be suspected and evaluated. This patient was overlooked on that part when patch closure of ruptured sinus of valsava was performed. An anomalous origin of coronary artery can be classified as follows; 1) absent left main trunk, 2) anomalous location of coronary ostium within aortic root or near proper aortic sinus of valsalva (for each artery), 3) anomalous location of coronary ostium outside normal "coronary" aortic sinuses, 4) an-omalous origination of coronary ostium from opposite, facing "coronary" sinus and 5) single coronary artery.10) This patient showed an anomalous location of the coronary ostium outside the normal "coronary" aortic sinuses (i.e., ascending aorta). Anomalous origin of the RCA may have clinical consequences such as angina pectoris, a myocardial infarction, syncope and sudden death. The pathologic mechanism is unclear but the usual explanation is mechanical com-pression of the RCA by great vessels, the aorta and the pulmonary artery. Additionally, an abnormal slit-like RCA ostium in the aortic wall and acute angulation of the RCA can lead to these pathologic results. Hutchins et al.5) suggested that the unusual angle of take-off and the more tortuous course of the proximal portion of the anomalous coronary artery can accelerate the rate of atherosclerosis. Laurence et al.11) suggested that the junction point of bound portion and the free portion of an anomalous artery as it wraps around the aorta is an area that is susceptible to lipid accumulation. These mechanisms can explain the obstructive lesion in the coronary artery of this patients. Clinically, however, angiographic documentation of anomalous coronary anatomy has not led to any effective or widely agreed recommendations for treatment so far. Though this patient is still quite well a year after PCI, we should undergo long term observation to clarify the influence of empirical intervention. When performing PCI, the operators and catheterization laboratories have to be aware of this anomaly and prepare specialized guiding catheters to facilitate PCI. Because of the technical difficulties during performing CAG, we performed 64 channel MDCT. Prior to PCI, MDCT-guided information is helpful in selective cannulation and intervention. Also, IVUS investigation of anatomical and functional features of the intussuscepted proximal ectopic segment in such cases may enable the identification of patients who need interventional treatment. We report here a case of anomalous origin of RCA arising from the ascending aorta with a history of open heart surgery and successful PCI guided by MDCT and IVUS.




 XML Download
XML Download