

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Case
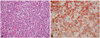
A 63 year old female without any previous medical history presented with an acute onset of dyspnea and facial swelling for 1 month duration. Physical examination showed that jugular venous engorgement was worse in the right decubitus position and we detected a cardiac systolic murmur (grade 3/6) and a third gallop. Tenderness on the right upper quadrant was noted and there were decreased breathing sounds in both lungs. The electrocardiography showed sinus tachycardia and a normal QRS axis. On laboratory findings, lactate dehydrogenase was remarkably elevated to 1,549 IU/L and the blood count was normal. Transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) revealed bi-atrial masses that were protruding into the ventricles with cardiac motion (Fig. 1A and B). The chest computed tomography (CT) scan showed right inferior pulmonary artery thromboembolism and both pleural effusion and huge biatrial masses. The mass extended to the superior vena cava (Fig. 2A and B). Cardiac CT showed huge bi-atrial masses and invasion into the atrial septal wall, myocardium and pericardium. We planned to do surgical resection and biopsy. The preoperative coronary angiography showed no stenotic lesions and there were feeding vessels from the right coronary artery and left circumflex artery to the biatrial masses (Fig. 1C and D). A median sternotomy was made, but surgical resection was not done except for biopsies because the myocardium was rigid due to tumor invasion to the pericardium and myocardium. The pathologic examination showed that the tumor was CD20 (+), CD79a (+), CD3 (-) and CD5 (-), and this was consistent with a diffuse large B cell lymphoma (Fig. 3). Positron emission tomography-CT (PET-CT) showed a markedly increased fluorodeoxyglucose (FDG) uptake in the heart and pericardium as well as mediastinal and right supraclavicular lymph nodes invasion (Fig. 2C). She was treated with rituximab, cyclophosphamide, adriamycin, vincristine and prednisone (R-CHOP). Follow-up TTE and TEE after the six rounds of chemotherapy revealed remnant, 1 cm sized, small, bi-atrial masses and reduced right and left heart failure (Fig. 4).
However, follow-up PET-CT after the end of R-CHOP chemotherapy showed no FDG uptake in the heart except for FDG uptake of resection scar and a lung abscess that occurred during chemotherapy (Fig. 3). After 1st line chemotherapy, she was followed up on out patient department. After therapy for a lung abscess, we plan to try 2nd line chemotherapy.
Discussion
The currently accepted definition of PCL is non-Hodgkin's lymphoma involving only the heart or with the bulk of the tumor located in the heart. PCL is a rare malignancy in immunocompetent patients.1-4) Its incidence has been increasing in immunocompromised hosts,5) and the main sites of involvement of PCL are reported to be the right atrium, right ventricle, myocardium and pericardium,1-4) and less often the left atrium and left ventricle.6) Furthermore, biatrial involvement is extremely rare.7)11-17) Right-sided involvement predominates in PCL in contrast to left-sided predominance in atrial myxoma, which is a major primary benign cardiac tumor. We report here a case of PCL that involved both atria in an immunocompetent patient. Ikea et al.6) reviewed the cardiac lymphomas that had been reported in the literature between 1995 and 2002. Here, we review cases of PCL with biatrial involvement reported between 1995 and 2008 (Table 1).
In the present case, the patient presented with right heart failure and symptoms like a superior vena cava syndrome. In the literature, the majority of PCL patients showed various and nonspecific symptoms such as dyspnea, edema, arrhythmia, cardiac tamponade, palpitation, and congestive heart failure. This appears to be correlated to a certain extent with the location of the neoplasm within the heart.
Most of the patients described in the literature were older patients with a nearly equal gender distribution. Diagnosis of a cardiac tumor was made on examination of the surgically resected specimen, and in earlier reports the diagnosis was also usually made postmortem. Pathology-based diagnosis of malignant lymphoma is essential in order to administer appropriate therapy. Most PCLs in the literature were B-cell neoplasms and of the diffuse large cell type.1-4)7-9) Our patient was also diagnosed with diffuse large B cell lymphoma and this was confirmed by immunohistology. The cells were CD20 B positive and CD3 T negative (Fig. 3). Modern imaging modalities helped make an early diagnosis and determine the extent of tumor involvement in the heart. In the present case, cardiac CT showed a huge, biatrial mass that extended through the atrial septum. The mass had a butterfly shape with a bigger right "wing" (Fig. 2D).
In conclusion, we reviewed the present case and seven patients with PCL with involvement of both atria reported between 1995 and 2008. PCL with involvement of both atria is due to a massive cardiac tumor and has a relatively poor prognosis as complete remission was obtained in only three of the eight patients.




 XML Download
XML Download