

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Marfan syndrome is an inherited connective tissue disorder. A number of patients with Marfan syndrome eventually undergo surgical correction of cardiovascular systemic involvement of the disease with not infrequent and various unexpected post-operative complications. We herein report a case of newly developed aortic dissection after aorta cannulation during mitral valve surgery in a patient with Marfan syndrome.
Case
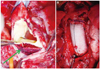
A 61-year-old Asian woman with Marfan syndrome (Fig. 1A, B and C) underwent a planned mitral valve surgical procedure due to symptomatic severe mitral regurgitation {New York Heart Association (NYHA) class III/IV} (Fig. 1D and E). She had no prior medical history of hypertension or diabetes mellitus. Preoperatively, her kidney and liver functions were normal. Chest roentgenogram revealed mild cardiomegaly but no active lung disease. An electrocardiogram revealed a sinus rhythm with non-specific ST-segment and T wave changes. For surgical treatment of mitral valve disease, an ascending aorta cannulation was performed for cerebral protection during cardiopulmonary bypass (CPB). Pre-operatively, the patient had no evidence of aortic dissection on transthoracic echocardiography (TTE) and computed tomography (CT) (Fig. 2A and C). The cardiac surgery was completed successfully and the patient was stable during the immediate post-operative period. The aorta was screened with intraoperative transesophageal echocardiography before and after CPB, which revealed no significant aortic disease. However, routine TTE carried out for evaluation of cardiac performance 1 day post-operatively revealed a dissecting flap at the ascending portion of the thoracic aorta (Fig. 2B). Therefore, CT was performed for full evaluation of aorta pathology, which revealed a newly developed aortic dissection involving the entire aorta (Stanford type A) (Fig. 2D). The patient underwent a second operation for the unexpected aortic dissection (Hemiarch replacement and the Bentall procedure) 1 day after the mitral valve surgery for stabilization, which was successful (Fig. 3). The dissecting flap and entry site of the aortic dissection at previous cannulation site on the ascending aorta was observed during the operation (Fig. 3A). Three weeks later, the patient was discharged from our hospital in good general condition.
Discussion
Marfan syndrome is an autosomal dominant inherited connective tissue disorder caused by a fibrillin-1 gene mutation with a prevalence of 1 in 5000-10000 individuals.1) The condition is associated with involvement of the cardiovascular system, along with the skeletal, ocular, and respiratory systems, in addition to other tissues such as skin, integument, and dura mater.2) Approximately 77% of patients with Marfan syndrome have major cardiovascular involvement such as valve disease and aortic pathology,2) a considerable number of whom eventually need surgical correction. Our patient had severe mitral regurgitation and underwent a mitral valve repair, where the mitral valve operation itself was successful.
The main pathophysiology of Marfan syndrome is the disordered incorporation of fibrillin into connective tissue, while media of the vascular wall is prone to cystic medial necrosis and vacuolization.3) Aortic involvement in Marfan syndrome can cause aortic dissection and/or rupture, which are common causes of premature death.4) There was no evidence of aortic disease in our patient based on pre-operative imaging studies. However, aortic cannulation during CBP could have injured the aortic wall, which may have been an initiating factor for the newly developed aortic dissection. Aortic dissection is a probable complication after aorta cannulation during CBP and the threatening condition associated with aortic injury during percutaneous interventional procedure has been reported in patients who underwent supra-aortic debranching and endovascular stenting of the aortic arch and the descending aorta.5) Moreover, Kumar et al.6) reported an interesting case of an iatrogenic acute dissection of Marfanoid aorta after cardiac surgery. The case was notable because the location of the intimal tear was not the directly manipulated site. Therefore, it can be said that patients with Marfan syndrome have existing subclinically disordered aorta wall tissue, even without significant findings on currently available cardiovascular imaging modalities. At the same time, fluctuating cardiac performances during the post-operative period and cardiotonic agent use after cardiac surgery may be contributing factors for disastrous conditions in patients with Marfan syndrome in whom the aortic wall is weak and friable.
Our case strongly suggests that aorta cannulation should be carried out with caution during cardiac surgery in patients with Marfan syndrome and appropriate imaging studies, including echocardiography to survey probable complications of aorta cannulation, should be performed after surgery. Concurrently, strict hemodynamic monitoring and appropriate cardiac performance control must be applied in the post-operative period until the cannulation site is completely healed.


 XML Download
XML Download