

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite a paucity of data supporting their safety and efficacy, the use of heterogeneous overlapping drug-eluting stents (DESs) is not uncommon for treating diffuse long lesions in clinical practice.1)2) Therefore, clinical trials and basic studies are needed to fully clarify their safety and efficacy and identify the potential pathophysiological mechanisms. Additionally, we suppose that the implantation sequence of different DESs may have distinct impacts on the endothelialization and arterial responses, particularly at the overlapping stented segment. Thus, in the present study, we evaluated the impacts of different implantation sequences of heterogeneous overlapping DESs on the endothelialization and arterial responses in rabbit iliac arteries.
Materials and Methods
Animal study protocol
Twenty-one New Zealand White rabbits, weighing 4.14±0.37 kg, were randomly assigned to receive two overlapping bare-metal stents (BMS, Driver™, Medtronic AVE Co., Minneapolis, MN, USA) (group I, B+B, n=7), or distal sirolimus-eluting stent (SES, Cypher™, Cordis Corp, Johnson & Johnson Co., New Brunswick, NJ, USA) plus a proximal paclitaxel-eluting stent (PES, Taxus™, Boston Scientific Co., Natick, MA, USA) (group II, C+T, n=7), or distal PES plus proximal SES (group III, T+C, n=7). After being anesthetized with ketamine (20 mg/kg intramuscularly) and xylazine (2 mg/kg intramuscularly), the stents were deployed at a single iliac artery via a right carotid artery approach under fluoroscopic guidance. The diameters of the stents were determined according to the iliac artery diameter after nitroglycerine infusion with a ratio of stent to artery of 1.0 to 1.1. Individual stents were deployed at their respective nominal pressures (9-11 atm, 10-second balloon inflation), and the overlapped segment was postdilated at 12 atm to ensure complete expansion.
All rabbits were pretreated with aspirin 40 mg PO (-10 mg/kg) and clopidogrel 25 mg PO (-6 mg/kg) 24 hours before stenting with continued therapy (same doses of aspirin and clopidogrel) until death. Additionally, unfractionated heparin (150 IU/kg) was administered intravenously before catheterization procedures. This animal study was approved by the Ethical Committee of Korea University Guro Hospital, Seoul, Korea.
Follow-up angiography and acetylcholine provocation test
Animals were anesthetized 3 months after the index procedure, and follow-up angiography of the iliac arteries was performed to evaluate the angiographic outcomes including the presence of stent fracture, patency, and position of the overlapping stents.
Endothelial function of the stented iliac artery was assessed after direct arterial infusion to iliac arteries using increasing doses of acetylcholine (ACh) (3, 6, and 15 µg/min) followed by nitroglycerin via a microcatheter. ACh was injected into the stented iliac artery over a 1 minute period with 5 minutes intervals.3) Angiography was repeated after each ACh dose. Then, an intrailiac infusion with 0.2 mg nitroglycerin was administered, and angiography was performed 2 minutes later. If significant vasoconstriction of the iliac artery was induced with any ACh dose, the ACh infusion was stopped. Significant endothelial dysfunction was defined as a transient >90% luminal narrowing of the stented iliac artery.3)4)
Subsequently, rabbits were euthanized with an overdose of ketamine, and the stented arteries were perfusion fixed in situ. Specimens were embedded in 10% formalin; and 3 mm from the proximal segment, middle overlapped segment, and distal ends of the stent were cut with a tungsten carbide knife (Delaware Diamond Knives, Wilmington, DE, USA). Sections were cut on an automated microtome (Leica) and stained with hematoxylin and eosin.
Histopathological analysis
All histological samples were managed blindly by an expert. Computerized planimetry was performed as described previously.5)6) Specimens were embedded in methylmethacrylate, and 50-100 µm sections were cut approximately 1 mm apart with a low-speed diamond wafer mounted on a Buehler Isomet saw (Buehler Ltd., Lake Bluff, IL, USA), leaving the stent wires intact in the cross-sections to minimize potential artifacts caused by removing stent wires.
A calibrated microscope digital video imaging system, and a microcomputer program (Visus 2000 Visual Image Analysis System) were used to measure the sections. Lumen area borders were manually traced, and the area was circumscribed by the internal elastic lamina and the innermost border of the external elastic lamina (external elastic lamina area). The measured internal elastic lamina area minus the lumen area was considered the neointimal area. Area stenosis was calculated as 100×{1-(lesion lumen area/lesion internal elastic lamina area)}.5) The measurements were made on four cross-sections of each stent.
Arterial injury at each strut was evaluated by the anatomic structures that penetrated each strut. A numeric value was used as previously described by Schwartz et al.7): 0=no injury; 1=break in the internal elastic membrane; 2=perforation of the media; 3=perforation of the external elastic membrane to the adventitia. The injury score was calculated by dividing the sum of each inflammatory score by the total strut number at the examined section.5)6)
To determine the inflammatory score for each individual strut, a grading system was used as follows: 0=no inflammatory cells surrounding the strut; 1=light, noncircumferential lymphohistiocytic infiltrate surrounding strut; 2=localized, moderate to dense cellular aggregate surrounding the strut noncircumferentially; and 3= circumferential dense lymphohistiocytic cell infiltration of the strut. The inflammatory score for each cross-section was calculated by dividing the sum of the individual inflammatory scores by the total number of struts in the examined section.6)8)
Statistical analyses
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) 11.0 (SPSS Inc., Chicago, IL, USA). Differences among groups of continuous variables were evaluated by one-way analysis of variance. Differences in discrete variables were expressed as counts and percentages and were analyzed with the chi-square (or Fisher's exact) test among groups as appropriate. Data are expressed as rate or mean±standard deviation. A two-tailed p of <0.05 was considered statistically significant.
Results
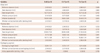
The baseline procedural characteristics were similar among the three groups (Table 1). The 3-month follow-up angiography of the distal stented segment after the index procedure showed that the B+B and C+T groups had significantly lower minimal luminal diameter (MLD), higher restenosis percentage, and late loss compared with those in the T+C group. The reference diameter and edge restenosis percentage were similar among the three groups. Interestingly, three cases of stent fractures occurred but only in the C+T group, whereas no stent fractures were observed in the other two groups. Furthermore, one rabbit with a stent fracture developed extensive necrosis distal to the fracture site (Fig. 1). No angiographic stent thrombosis was observed in the three groups at the time of angiographic follow-up. The three groups did not differ significantly in the proximal stented segment, including MLD, restenosis percentage, and late loss. No stent fracture or thrombosis was observed among the three groups. Similar results were observed in the overlapping segment (Table 2).
The histopathological results are presented in Table 3 and Figs. 2 and 3. Consistent with the 3-month angiographic outcomes, the B+B and C+T groups had significantly lower luminal area, lower internal elastic lamina (IEL) area, and higher area stenosis in the distal stented segment compared with those in the T+C group. The C+T group had significantly lower IEL area, and a trend toward lower luminal area compared with those in the B+B group. In addition, the C+T group had significantly higher injury and inflammatory scores due to the three cases of stent fracture compared with those in the T+C and B+B groups. Despite similar injury scores, the T+C group had significantly higher inflammatory scores in the distal stented segment than those in the B+B group.
The C+T and T+C groups had significantly larger luminal area and IEL area in the proximal stented segment compared with those in the B+B group. But, neointimal area and area stenosis did not differ significantly among the three groups. Furthermore, the injury and inflammatory scores were similar among the three groups.
The three groups did not differ significantly regarding luminal area, neointima area, IEL area, or area stenosis in the overlapping segment. Moreover, the three groups also had similar injury scores. But, the C+T and T+C groups had significantly higher inflammatory scores than those in the B+B group, consistent with the results in the distal stented segment.
The endothelial function assessed with the ACh provocation test showed that the C+T and T+C groups had a significantly higher incidence of significant vasoconstriction as compared with that in the B+B group, suggesting significant endothelial dysfunction in the vessels where DESs were deployed (Table 4). Significant iliac artery spasm (luminal narrowing >90%) was induced with ACh infusion (50 µg/min) (Fig. 4A), and vasodilation was achieved after a nitroglycerine infusion (Fig. 4B).
Discussion
As the overall angiographic outcomes and histopathological results were comparable between the two groups with different first-generation DES implants (Cypher and Taxus) at three different stented segments (proximal, overlapping and distal), the present study did not support the hypothesis that the different implantation sequences of heterogeneous DESs have distinct impacts on the endothelialization and arterial responses in the rabbit iliac artery.
Some studies have shown that deploying BMSs for diffuse long lesions is associated with a high restenosis rate.9) DESs have significantly reduced the rate of restenosis by inhibiting neointimal hyperplasia after stenting. However, a diffuse long lesion still remains an independent risk factor for restenosis even in the DES era.10) Therefore, a variety of methods have been tested to treat diffuse long lesions including the heterogeneous overlapping DES.1)2)11)12) Kang et al.1) evaluated the effect of stent overlap with different DESs on neointimal hyperplasia in 47 patients with diffuse long lesions. Their study showed that percutaneous coronary intervention with different overlapping DESs resulted in similar suppression of neointimal hyperplasia and did not increase the side effects of the DES compared with using the same overlapping DES. Similarly, a recent study also suggested that overlapping heterogeneous DESs and overlapping homogeneous DESs had similar long-term safety and efficacy in patients with diffuse long lesions.2) A preclinical study in a porcine model reported that overlapping different DESs did not differ significantly from overlapping the same DES in terms of restenosis rate, neointimal area, and endothelialization scores.5) However, only one group of heterogeneous overlapping stents was used in their study.5) It still remains unclear whether the implantation sequences of heterogeneous overlapping DES influences endothelialization and neointimal hyperplasia. Therefore, our study was the first to test this question and showed that although the two overlapping DES groups had significantly smaller neointimal area and less late loss compared with those in the BMS group, the two overlapping DES groups did not differ significantly, suggesting that the different Cypher and Taxus implantation sequences had similar effects on neointimal hyperplasia.
Concerns have been raised regarding the safety of DESs. Some studies have shown that DESs result in a higher incidence of stent thrombosis compared with BMSs even long after the index procedure.13) Increasing evidence suggests that the local inflammatory reaction in the DES segment might be an important mechanism behind stent thrombosis.14)15) Nakazawa et al.14) showed that DES implantation in the culprit lesion of acute myocardial infarction is associated with delayed arterial healing and increased local inflammatory reactions, which increase the rate of late stent thrombosis. Cook et al.15) demonstrated that very late stent thrombosis is associated with histopathological signs of inflammation. Some preclinical studies have also revealed that DESs are related to significantly higher inflammatory reactions in the stented segment as compared with those in BMSs.5)16)17) Finn et al.16) compared the histopathological response at sites of overlapping homogeneous SESs, PESs, and BMSs in the rabbit iliac artery. Their study showed that DESs are associated with delayed arterial healing and promote inflammation at overlap sites compared with those of BMSs, suggesting that patients receiving overlapping DESs need more frequent follow-up than patients with overlapping BMSs. In addition, a study by Lim et al.5) also suggested that although DESs inhibit neointimal hyperplasia, significantly higher inflammation reactions and poorer endothelialization occur at the site of overlapped segments as compared with those of BMS. Consistent with these studies,5)16)17) our study also suggested that implanting overlapping DESs was related to significantly higher inflammatory reactions in the overlapped segment as compared with those in BMS. Specifically, our study also revealed that the local inflammatory reactions did not differ significantly by implantation sequence of the different DESs.
Furthermore, some studies have suggested that DES implantation is associated with significant endothelial dysfunction compared to that of BMSs.18) Similarly, our study showed that the two DES groups had a higher incidence of significant iliac artery spasm as compared with that in the BMS group, suggesting that a higher prevalence of endothelial dysfunction occurred in the DES implanted segment. Given the higher inflammatory scores observed in the two DES groups, we suppose that the long-lasting inflammatory reactions at the DES stented segments might be the mechanism behind the significant endothelial dysfunction in the DES groups.
Interestingly, three cases of stent fracture occurred at a site distal to the Cypher segment. These fractures might have developed due to active joint motion in the area of the iliac artery. Recently, special attention has been paid to the clinical implications of stent fracture. Chhatriwalla et al.19) reviewed literature regarding DES fracture and showed that most DES fracture reports involved Cypher stents, and that a DES fracture could be associated with stent thrombosis, myocardial infarction, or angina. Due to the potentially harmful effects of stent fracture, we suggest that a more flexible DES should be used in an artery with a greater range of motion such as the mid right coronary artery. Notably, the Cypher and Taxus stents did not differ significantly regarding endothelialization, neointimal growth, or arterial response at the proximal and overlapped segments, suggesting that the effect of inhibiting neointimal hyperplasia and peristructural inflammation were similar between these two types of DESs. More neointimal hyperplasia and a greater arterial response in the distal segment of C+T was mainly due to the stent fractures.
Study limitations
The present study had some limitations. First, the number of experimental animals was relatively small, which might have weakened the conclusions. Second, we used first-generation DESs (Cypher and Taxus), and compared them with BMSs. Furthermore, we could not distinguish the effects of eluting drug from those of polymers. Third, we prepared the groups with the same overlapping DESs. Thus, the conclusions of the current study regarding the impacts of different implantation sequences on endothelialization and arterial response should be interpreted cautiously. Fourth, because the stents were deployed in normal iliac arteries, the results may not be representative of human atherosclerotic disease, particularly human coronary artery disease.
In conclusion, despite similar arterial injury, greater inflammatory reactions were observed in the DES overlapped segments regardless of the implantation sequence as compared with BMS. Moreover, DES was more associated with impaired endothelial function on the adjacent nonstented segments as compared with that of BMS. Therefore, more frequent clinical follow-up with intensive medical therapy will be needed in patients receiving overlapping DESs as compared with those receiving overlapping BMSs.






 XML Download
XML Download