

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Individuals with prehypertensive blood pressure (BP) have an increased risk of developing cardiovascular disease relative to those with optimal levels.1) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High BP (JNC 7) defined a new entity termed "prehypertension" to reflect the growing evidence that systolic BP (SBP) values between 120 and 139 mm Hg and diastolic BP (DBP) values between 80 and 89 mm Hg are associated with an increased cardiovascular risk.2) The European Guidelines,3) however, divide this population into two groups: those with SBP between 120 and 129 mm Hg or DBP between 80 and 84 mm Hg are classified as normal, whereas those with SBP between 130 and 139 mm Hg or DBP between 85 and 89 mm Hg are classified as high-normal. Although the association of cardiovascular risk with elevated BP is well-accepted,4) only a few studies have addressed the risks of major adverse cardiac events (MACEs) for the population with acute myocardial infarction (AMI) in the high-normal range. The importance of management in "high-normal BP" according to definition of European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) seems to be underemphasized. We presently investigated the impact of high-normal BP on adverse cardiac events in the patients with AMI from the Korea Acute Myocardial Infarction Registry (KAMIR).
Subjects and Methods
Methods
Korea Acute Myocardial Infarction Registry is a Korean, prospective, open, observational, multicenter, on-line registry of AMI with support from the Korean Society of Cardiology since November 2005. The 50 participating hospitals are capable of primary percutaneous coronary intervention (PCI). Details of the KAMIR have been published.5) AMI was diagnosed by characteristic clinical presentation, serial changes on electrocardiogram suggesting infarction, and increase in cardiac enzymes.6) ST-segment elevation myocardial infarction (STEMI) was defined by new ST elevation in ≥2 contiguous leads, measuring >0.2 mV in leads V 1-3, or 0.1 mV in all other leads.
Demographic and clinical characteristics including age, gender, cardiovascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, smoking status, and family history of coronary heart disease) and co-morbidities were identified. Hypertension was defined as previously diagnosed by a physician and/or receiving medication to lower BP. Hyperlipidemia was defined as previously diagnosed by a physician and/or receiving lipid-lowering drugs. Family history of coronary heart disease was defined as coronary heart disease in first-degree male relative <55 years old or coronary heart disease in first-degree female relative <65 years old. Height, weight, and body mass index (BMI) were measured at admission. Initial vital signs were measured and Killip class was evaluated at admission. Electrocardiogram was recorded and analyzed in all patients by attending physicians and/or cardiologists. Blood samplings for baseline laboratory tests except lipid measurement were collected at admission or before PCI. Overnight fasting blood was also sampled for lipid levels. The left ventricular ejection fraction was determined by two-dimensional echocardiography during the index hospitalization. In-hospital complications and their management were also recorded.
Initial treatment strategy for patients with STEMI could include PCI, thrombolysis, or conservative treatment at the discretion of the attending physician. Primary PCI was defined as emergency PCI performed within 12 hours after admission or PCI in patients with continuing symptoms or cardiogenic shock, even after 12 hours. For patients with non-STEMI, initial treatment strategy could include early invasive PCI or conservative treatment based on current guidelines, at the discretion of the attending physician. Early invasive PCI was defined as emergency PCI that was performed within 48 hours in patients with non-STEMI with remaining symptoms. Glycoprotein IIb/IIIa receptor blockers, thrombectomy devices, predilatation balloons, and stents during index PCI were used at the decision of the interventional cardiologists. Epicardial coronary blood flow in the infarct-related artery before and after stent implantation was graded according to the classification used in the Thrombolysis in Myocardial Infarction (TIMI) trials. Successful PCI was defined as a residual stenosis <50% in diameter with final TIMI grade 3 flow. Furthermore, prescription of optimal evidence-based medications was encouraged in all indicated patients who had no contraindications to guideline-recommended drugs during index hospitalization or after discharge.
Patient population and end point
From November 2005 to May 2009, 14871 patients with a final diagnosis of AMI were enrolled in KAMIR. Of these patients, to avoid effects of autonomic nerve system, patients without history of hypertension, present angina, present dyspnea, present bradycardia, and tachycardia were analyzed in this study. BP was measured with a practical manual for usual emergency rooms. Usually, these were single-measured values. There was no limitation of hypotension and the lowest SBP among them was 120 mm Hg. Present angina and dyspnea were defined according to patients subjective symptoms upon arrival at the emergency department. Bradycardia was defined as <60 beats/min. Tachycardia was defined as >100 beats/min.
Among the 14871 patients, 159 patients (61±12.3 years, 122 males) satisfied the study inclusion criteria. We analyzed MACEs including death, recurrent myocardial infarction, revascularization including repeat PCI (target lesion or target vessel revascularization, or non-target vessel revascularization), and coronary artery bypass grafting in patients with normal BP (group I, n=78) and high-normal BP (group II, n=81) according to ESH 2007 definition.3) Cardiac death was defined as death from pump failure, arrhythmia, or mechanical complications including ventricular septal rupture and free wall rupture. Follow-up data were obtained by reviewing medical records and/or telephone interview with patients. All data were entered into an electronic web-based case-report form.
Statistical analyses
Continuous variables were presented as the mean value±SD, comparisons were conducted by 2-tailed Student's t-test. Discrete variables were presented as percentages and relative frequencies and comparisons were conducted by chi-square statistics or Fisher's exact test as appropriate. Logistic regression analysis was performed to identify the independent predictors of MACEs with a 95% confidence interval (CI). The Kaplan-Meier method was used to estimate the risk of MACEs up to about 360 days, stratified by normal or high-normal BP. The Statistical Package for the Social Sciences (SPSS) for Windows, version 15.0 (SPSS Inc., Chicago, IL, USA) was used for all analyses. The level of significance for this study was 0.05.
Results
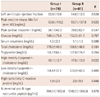
Among 14871 patients, 159 patients (61±12.3 years, 122 males) satisfied the study incision criteria. Group I had 78 patients (60.9±12.4 years). Group II had 81 patients (61.6±12.5 years). BP of group I was 120±1.6/77±6.3 mm Hg. BP of group II was 130±2.0/82±7.7 mm Hg. BP of group II was higher (p<0.001). However, at discharge, there was no statistical difference of BP (group I=116±10.7/73±7.9 mm Hg, group II=113±20.1/75±9.2 mm Hg, p=0.389). Baseline clinical characteristics and initial presentation of patients are listed in Table 1. There were no significant differences in demographics, initial presentation, and vital signs.
Past medical histories were not different (Table 1). The prevalence of diabetes, dyslipidemia, smoking history, familial history, and BMI were not different between groups. STEMI was 43.6% of group I and 44.6% of group II.
Baseline laboratory characteristics are listed in Table 2. Left ventricular ejection fraction, levels of peak creatine kinase-Mo full term myocardial bind, serum creatinine, high-sensitivity C-reactive protein, and N-terminal pro-B-type natriuretic peptide did not different. The level of total cholesterol was not different, but the level of high density lipoprotein-cholesterol was higher in group II (43.1±12.7 mg/dL vs. 47.8±13.9 mg/dL, respectively; p=0.032).
Initial treatment strategy and discharge medications were not different (Table 3).
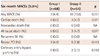
The angiographic and procedural data are shown in Table 4. Left main coronary artery disease and three-vessel disease were not different between groups. There were no significant differences between groups in number of left anterior descending coronary artery. There were no significant differences between groups in lesion types of American College of Cardiology/American Heart Association criteria. Initial TIMI flow grade was better in group II. Final TIMI flow grade was not different. The deployed stent profile, such as type, length, and diameter were not different between groups. Door to balloon time was not different. PCI success rate was not different.
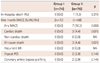
In-hospital death occurred in 0 (0.0%) vs. one (1.3%) patient (p=0.319). One-month composite MACE occurred in zero (0.0%) vs. seven (10.3%) patients (p=0.006) (Table 5). The latter seven included three (4.4%) cardiac deaths, two (2.9%) repeat PCIs, and two (2.9%) coronary artery bypass grafts. Six-month clinical follow-up rate were 88.9%. Thirteen (9.9%) developed MACE 6 months after the index treatment. Six-month composite MACE occurred in three (4.4%) vs. 10 (15.6%) patients (p=0.031) (Table 6). The former three (4.4%) were repeat PCIs.
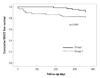
The later 10 included three (4.7%) cardiac deaths, five (7.8%) repeat PCIs, and two (3.1%) coronary artery bypass grafts. One-year clinical follow-up rate were 85.8%. Seventeen (13.6%) developed MACE 1 year after the index treatment. The former six included one (1.5%) cardiac death, four (6.0%) repeat PCIs, and one (1.5%) coronary artery bypass graft. The later 11 included 3 (5.2%) cardiac deaths, six (10.3%) repeat PCIs, and two (3.4%) coronary artery bypass grafts. Cumulative MACEs-free survival was better in group I than in group II (p=0.049) (Fig. 1).
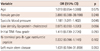
Compared with group I, the odds ratio for group II was 1.181 (p=0.045, 95% CI, 1.011-1.402) for 6-month composite MACEs (Table 7). In multivariate logistic regression analysis, SBP was independent of age, gender, diabetes mellitus, familial history of coronary heart disease, N-terminal pro-B-type natriuretic peptide, and left main stem disease, as a predictor of MACEs at 6 months after AMI. However, group II did not have statistical significance to predict 12-month composite MACE.
Discussion
We analyzed MACEs after AMI in patients with normal BP and high-normal BP. Baseline status was very similar in both groups. Treatment strategy and medication was not different between groups. The patients with high-normal BP had more MACEs and poor survival 6 months after index treatment.
The United States is facing a serious challenge in the prevention and management of prehypertension and hypertension. People's awareness and control of hypertension remain poor.7) High-normal BP is common and is associated with increased vascular mortality. The results of a multiple ethnic groups investigation has demonstrated that high-normal BP is a risk factor for incidence of coronary heart disease in both men and women.8) In a Japanese cohort study, high-normal BP was revealed to be a risk factor for the incidence of stroke and MI in the general urban men population.4) The extent to which it increases risk of cardiac death, recurrent MI, repeat PCI, and coronary artery bypass grafting after treatments of AMI is not clear. Some investigators reported that pre-hypertension appeared to be associated with an increased risk of MI and coronary artery disease but not stroke.9) Some study reported that at 6-month follow-up, age- and gender-adjusted odds ratios for adverse events were equivalent in hypertensives and normotensives after an initial acute coronary syndrome.10) The authors explained this interesting result with the fact that treatment for the patients with hypertension was better tailored. In our study, there were no differences in treatment strategy and discharge medications.
The main finding of this study was that the patients with high-normal BP, which was measured in the emergency room, have poor prognosis 6 months after index treatment. Interestingly, this study had a very well-conditioned baseline state comparable with prospective studies. Among the dozens of baseline parameters, only high density lipoprotein-cholesterol level was not statistically equal. Thus, this study does not need to be adjusted to reduce confounding variables. Even though group II had generally better known prognostic factors, such as higher high density lipoprotein-cholesterol, more single vessel diseases, and higher TIMI flow grade, group II had poor 6-month MACEs and poor survival curve. It shows that high-normal BP affects on prognosis more than lipid profile and angiographic findings. In other words, it shows that more delicate BP control is needed to prevent MACEs after AMI.
Antecedent hypertension interacts with age, neurohumoral activation, and early ventricular remodeling to confer greater risk of heart failure after MI.11) High-normal BP has also been associated with increased risk of carotid atherosclerosis.12) We think our results can be explained with the conclusion that the patients with tightly controlled BP have less progression of atheroma than the patients without tightly controlled BP. Sipahi et al.13) compared the effects of normal, pre-hypertensive, and hypertensive BP levels on progression of coronary astherosclerosis. In that report, those with hypertensive BP levels displayed an increase in atheroma volume on an arterial segment, those with pre-hypertensive BP levels had an intermediate outcome, and those with normal BP levels had a trend for atheroma regression. Patients who improved from a pre-hypertensive BP level at baseline to normal BP levels during the study had significantly less progression of atheroma than patients who remained pre-hypertensive. That study suggested that in patients with coronary artery disease, the optimal BP goal may be substantially lower than 140/90 mm Hg as BP levels may have a negative correlation with atheroma progression.13) We suggest that benefits can be obtained by controlling high-normal BP more tightly in patients with coronary artery diseases.
Medications including beta blockers, ACE inhibitors, and angiotensin converting enzyme inhibitors are needed for better prognosis after AMI. In some studies, administration of amlodipine to patients with coronary artery disease and normal BP resulted in reduced adverse cardiovascular events. Directionally similar, but smaller and not significant, treatment effects were observed with enalapril. For amlodipine, intravascular ultrasound showed evidence of slowing of atherosclerosis progression.14) In our study, treatment strategy and medication was not different between groups.
In patients with hypertension and diabetes or renal disease, the BP goal is <130/80 mm Hg according to JNC7.2) The target BP goal is <130/80 mm Hg in diabetics and in high or very high risk patients according to the ESC and ESH 2007 guidelines.3) What should we do for high risk patients without definite hypertension, in case of prehypertension according to JNC7 and normal or high-normal hypertension according to ESC/ESH 2007, especially after AMI? Even though high-normal BP patients had better baseline clinical situation, follow-up MACE was poorer in the KAMIR patients than in patients with normal BP. This seems to confirm the importance of BP control in high-normal BP patients. The therapeutic BP target goal for the high-normal BP patients with AMI should be <140/90 mm Hg, which is recommended in JNC7 and should be as low as 130/80 mm Hg according to the ESC and ESH 2007 guidelines, even though the patients do not have definite hypertension.
Even though this study population was relatively small, the patients characteristics were very similar to the total KAMIR population, which is revealed by similar MACEs rate to total population.15) Total 6-month MACEs rate was 8.0% and our 6-month MACEs rate was 9.8%. When one-month MACEs were excluded, there was no difference of 6-month and 1-year MACEs. These findings are compatible with a previous report about KAMIR.15) According to that report, initial in-hospital instabilities such as shock and angiographic severity were responsible for 6-month MACEs. In other words, one-month MACEs affect 6-month MACEs. Also, baseline characteristics between the groups were similar enough to require no adjustment. Thus, those characteristics could overcome study limitation such as small study population number. Finally, we believe that high normal BP, which was measured in the emergency room, could predict 6-month MACEs dependently of 1-month MACE.
Our study has several other limitations. The study was based on a single measurement of BP, which may lead to a mis-classification of BP levels. It is more appropriate to compare BP management during follow-up to reduce bias related to BP measurement. Actually, we had compared BP at discharge. There was no difference between groups, perhaps as a result of a similar effort to control MI using angiotensin converting enzyme inhibitors or angiotensin receptor blockers, calcium channel blockers, and beta blockers, as several options. Even though there was no difference of BP after management, the prognosis was different. So, it may be valuable to evaluate initial BP in the emergency room. To avoid effects of autonomic nerve system, we enrolled patients without present angina, present dyspnea, present bradycardia, or tachycardia. Thus, we could have small number of population. So, those filters in patient selection might cause selection-bias in analysis. One-year clinical follow-up rate was 85.8% in this study.
Conclusively, although high-normal BP patients had better baseline clinical situation, follow-up MACEs were poorer in KAMIR than patients with normal BP. It shows that high-normal BP has adverse impacts on cardiac events in AMI. Therefore, strict BP controls are needed to prevent adverse cardiac events after AMI.



 XML Download
XML Download