

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Malignant melanomas are tumors with the highest rates of cardiac metastasis. However, cardiac metastasis is diagnosed in less than 1% of patients with malignant melanoma because less than 10% of these patients present with cardiac symptoms.1-3)
Identification of cardiac metastasis from melanoma usually means that the patient is suffering systemic metastasis. Unlike typical cardiac metastasized patients, we report a first case of a patient with a metastatic malignant melanoma in the heart without an identifiable primary source or additional metastasis in Korea.
Case
A 59-year-old woman was admitted for cough and pleuritic chest pain with no history of malignancy or heart disease. Her initial blood pressure was 110/70 mm Hg, pulse rate 70 beats/min, respiratory rate 20/min, and body temperature was 36.1℃.
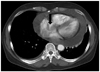
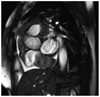
Jugular veins were not distended. No hepatomegaly or audible cardiac murmurs were present. Laboratory studies, including a complete blood count, liver, and chemical profiles were in normal ranges. Electrocardiography revealed a normal sinus rhythm. Chest radiography showed cardiomegaly without abnormal lesions in bilateral lung fields. Chest computed tomography showed a large amount of pericardial effusion and a mass in the right atrium (RA) (Fig. 1). Transthoracic echocardiography showed a large mass measuring 42×31 mm in the RA, which did not obstruct tricuspid valve flow. Her ejection fraction was normal (Fig. 2). Pericardiocentesis was performed. Effusion analysis showed a red blood cell count of 1.9×105/mm3 and a white blood cell count of 3300/mm3 (lymphocytes, 55%; neutrophils, 14%). No malignant cells in the pericardial fluid were noted. Cardiac MRI also revealed a large mass surrounding ascending aorta spread into transverse sinus and around pulmonary trunk (Fig. 3).
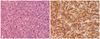
Instead of tumor resection, considering the risk of open heart surgery and poor prognosis of extensive cardiac metastasis, pericardial window operation and epicardial mass biopsy were performed to relieve symptoms and confirm the pathological diagnosis. Pathological analysis including immunohistochemistry revealed the final diagnosis to be malignant melanoma (Fig. 4). The primary cutaneous melanoma could not be identified despite careful dermatological examination. The patient had no history of halo nevus or mole removal. Positron emission tomography revealed no other distant organ metastasis except for heart and mediastinal lymph nodes.
Discussion
Malignant melanoma has aggressive biological behavior and the greatest tendency for metastasis to the heart.1) Although autopsy studies reported an incidence of 50% to 71%, cardiac metastasis is diagnosed in less than 1% of patients with malignant melanoma because less than 10% of these patients present with cardiac symptoms.2) Such metastases most frequently occur after multifocal hematological dissemination and may develop anywhere in the heart.3) Melanotic metastases can invade the wall of any of the 4 cardiac chambers, and the RA is involved most frequently.4)
The clinical signs and symptoms of cardiac metastasis are unclear and non-specific, although when present, the clinical signs and symptoms include fatigue, weakness, pericardial effusion, congestive heart failure, cardiac arrhythmia, superior vena cava syndrome, right ventricular outflow and inflow obstruction, and transient ischemic attack.5) However, patients with malignant melanoma who have cardiac metastases may present symptoms only caused by tumors in other organ systems. Although cardiac involvement occurs during the course of the disease, it is rare that the initial manifestation is cardiac metastasis.
A tumor's anatomic location and extent of invasion determine the feasibility of surgical intervention, which should optimally be performed during the early stages of the disease.6) A complete resection of an intracardiac melanoma prevents potential morbidities that are associated with progressive intracardiac growth, such as superior vena cava syndrome, right ventricular outflow and inflow obstruction, dysrhythmia, cardiac tamponade, and heart failure.6) Even when total resection is not possible, conservative surgery can relieve symptoms and prevent imminent cardiac failure. Conservative surgery improves the quality of a patient's life, as in our patient's case.
Although more than 90% of melanomas have a cutaneous origin,7) melanomas may sometimes present metastatically in the absence of a primary lesion, termed melanomas of unknown primary origin. Most authors estimate that 2-6% of patients are diagnosed with metastatic melanoma of unknown primary site. In particular, such a metastatic melanoma in the heart such as in this patient without a known primary cutaneous origin is a rare presentation and chiefly an anecdotal finding of metastatic melanoma. Several reported cases can be found in the literature about cardiac involvement with cutaneous primary malignant melanoma and multiple metastasis in Korea, as well as worldwide.8)9) As far as we know, malignant cardiac melanoma without a primary origin has not yet been reported in Korea.
The survival of patients with unknown primary melanoma was demonstrated to be similar to that of patients with known primary tumors when corresponding stages were compared.10-12) Those patients with metastases to any other visceral sites are described to have a 1 year survival rate of 41% and a median survival of approximately 6 months.11)13)14) Accordingly, we expected that the outcome of this patient might be very unfavorable. Although total resection was not possible because of extensive cardiac metastasis, a pericardial window operation could resolve her symptoms.
After surgery, chemotherapy was planned, including cisplatin, dacarbazine, casmustine, and tamoxifen. However, the patient refused further chemotherapy after completion of two sessions. The patient has survived for 14 months after diagnosis. She is attending our hospital's outpatient oncology department.
As only few reports about cardiac metastasis of malignant melanoma without cutaneous origin have been published, we are uncertain if conservative surgery is associated with prolonged survival and if the role of surgery for survival is worth further investigation.

 XML Download
XML Download