

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dihydropyridine (DHP)-derivative calcium channel blockers (CCBs) are widely used as first-line antihypertensive agents.1) The currently known voltage-gated calcium channel subtypes include L-, T-, N-, P/Q-, and R-types.2) Efonidipine, a DHP-derivative CCB, has been proven to exert a blocking effect on L-type as well as T-type calcium channels.3) Recently, multiple actions of the T-type calcium channel have been noted, including regulation of the microvascular tone and firing rate of sinoatrial nodal cells in the heart,4)5)7) control over burst firing of thalamic neurons in relation to absence epilepsy,5)6) reduction in proteinuria and plasma aldosterone levels,2)8) and prevention of sudden death in mice with heart failure.9) Efonidipine has been clinically used in Japan as an antihypertensive agent for its mild persistent hypotensive effect. Despite the above mentioned pharmacological interests in efonidipine, its hypotensive action and effect on heart rate over an entire day have not been fully investigated. Patient with nocturnal hypertension have a worse prognosis than the ones with a normal circadian rhythm of blood pressure. Changes in the circadian blood pressure profile after the administration of an antihypertensive agent have direct implications on evaluating the quality of anti-hypertensive drug therapy.10)
In the present study, we examined drug-induced circadian changes in 24-hour systolic blood pressure (24-hour SBP) and heart rate (24-hour HR) obtained from 24-hour ambulatory blood pressure monitoring (24-hour ABPM) before and after treatment with efonidipine in patients with essential hypertension. Circadian variations of above parameters were expressed as a function of time. As the results, a quantitative analysis of antihypertensive action of the drug throughout the day can lead a new chronopharmacological approach on antihypertensive drug therapy.
Subjects and Methods
Participants and study design
A total of forty-five Japanese patients with hypertension (22 men and 23 women) who first visited the out-patient clinic of Showa University Fujigaoka Hospital, Yokohama, Japan, participated in this study. This group consisted of de novo hypertensive patients with an average age of 62.2±10.1 years, and all participants had either Grade 1 or Grade 2 essential hypertension according to the European Society of Cardiology guidelines for the management of arterial hypertension.1) The office SBP were between 140 and 179 mm Hg and diastolic blood pressure (DBP) were between 90 and 109 mm Hg, measured at least twice during a 2 week period; these measurements were performed during out-patient checkups after the patients were seated for at least 10 minutes. Conventional office BP measurements were always obtained by the same investigator who were technical cardiologists in order to avoid observer bias. Patients with secondary arterial hypertension, renal insufficiency, uncontrolled diabetes, and cardiovascular disorders including angina pectoris, congestive heart failure, chronic arrhythmia (e.g., persistent atrial fibrillation), or previous myocardial infarction, were excluded. After obtaining informed consent from the participants including the patients volunteer, the patients underwent 24-hour ABPM without treatment with antihypertensive drugs. After 24-hour ABPM, the subjects received 40 mg of efonidipine hydrochloride [5-(5,5-dimethy-l,3,2-dioxaphosphorinan-2-yl)-1,4-dihydro-2,6-dimethyl-4-(3-nitrophenyl)-3-pyridinecarboxylic acid, 2-{phenyl(phenyl-methyl)amino} ethyl ester, P-oxide, hydrochloride]; (Nissan Chem. Int. Ltd., Tokyo, Japan), which was administered once daily immediately after waking.11) This drug has been known as an L- and T-type CCB that exerts long-lasting antihypertensive action.11)12) If the attending physician determined that the voluntary blood pressure levels had normalized during the follow-up period after treatment, a second 24-hour ABPM was performed. If either the voluntary blood pressure or second 24-hour ABPM had not normalized for 3 months, efonidipine was replaced with another antihypertensive agent. The average follow-up period was 5.2±1.7 months. The ethics committee of Showa University Fujigaoka Hospital approved the protocol of this study.
24-hour ambulatory blood pressure monitoring assessment and actigraphy
The SBP and HR of each patient were automatically measured every 30 minutes for 24 consecutive hours from 9:00 a.m. to next 9:00 a.m. on the following day, using a cuff-oscillometric, multisensor ABPM device (TM-2425; A & D Co. Ltd., Tokyo, Japan), which simultaneously recorded blood pressure, electrocardiogram and physical activity during the entire 24-hour of a routine workday. The device satisfied the criteria of the Association for the Advancement of Medical Instrumentation and the British Hypertension Society. Previous reports have described the detailed features as well as the usefulness of this device in clinical hypertension research.13)14) The recording method using this device has authorized by related papers.14) The International Society of Hypertension recommends using recording intervals of 15- to 20 minutes during daytime and intervals of 30 minutes at night for 24-hour ABPM. However, most Japanese patients, particularly women, are unwilling to undergo SBP recording at short intervals (15- to 20 minutes) and decline to undergo 24-hour ABPM for a second time. Consequently, the SBP and HR were measured every 30 minutes. Hermida et al.'s15) criteria were used to evaluate whether the ABPM data series was valid for analysis. They commented that 24 hour-SBP data series were not considered valid for analysis if more than 30% of the measurements were missing, if data were missing for an interval of >2 hours, if data were obtained while patients had an irregular rest-activity schedule, or if the nighttime sleep period was 12 hours during ABPM. Eight patients who did not fulfill the criteria were excluded from this study. Actigraphy data and diary records were used to define wakefulness and sleep spans.
Diurnal to nocturnal systolic blood pressure ratio
In order to evaluate the effects of efonidipine on circadian rhythm, the diurnal and nocturnal mean SBP values (D/N SBP ratio) were studied. The average time at which the participants went to sleep in this study was 10:40 p.m., and the average time at which they woke up was 6:27 a.m. Accordingly, the diurnal period was derived as extending from 7:00 a.m. to 10:00 p.m., and the nocturnal period as extending from 10:30 p.m. to 6:30 a.m. The D/N SBP ratio was defined as the percentage decrease in SBP during nocturnal rest, relative to the diurnal mean SBP, and calculated using the following equation, (diurnal SBP mean-nocturnal SBP mean)/diurnal SBP mean×100.15)
If the D/N SBP ratio ranged from 10% to 20%, the 24-hour SBP mode was defined as dipper-type hypertension. If it ranged from 0% to 10%, the 24-hour SBP mode was defined as non-dipper-type hypertension.16)
The best-fit curve
A commercial computer program (MemCalc; Suwa Trust Co. Ltd., Tokyo, Japan) was applied to generate the best-fit curve for changes in the 24-hour SBP or HR (ΔSBP, ΔHR) every 30 minutes before and after administration of the drug. The best-fit curve was used to provide a more accurate assessment of the response to the action of the drug throughout a day. A detailed description of the program has been previously provided.17) This program primarily utilizes the maximum entropy method (MEM), which is applied to detect time structures in time-series data, and the non-linear least squares method (LSM) to provide a best-fit periodic function. Using this method, the pharmacokinetic characteristics of the drug can be expressed as precise numerical values. The median value shows the midline estimating statistic of rhythm (MESOR), which is the 24-hour average value of the rhythmic waveform function fitted to the data.
Results
The demographic characteristics and office blood pressure readings of the 45 subjects are shown in Table 1. All patients received an L- and T-CCB (efonidipine; 40 mg/day) after waking. The mean office SBP and DBP values of the participants were 165.1±11.0 mm Hg and 96.9±7.5 mm Hg, respectively. After treatment with efonidipine, the mean office SBP and DBP significantly dropped to 132.6±7.6 mm Hg and 80.1±6.8 mm Hg (p<0.01), respectively, and they were judged to be stable by the attending physician in the outpatient clinic.
According to the 24-hour ABPM assessment of Hermida et al.,15) 24-hour ABPM data series were not considered valid for analysis when more than 30% of the measurements were missing, and additionally when data were missing for an interval of >2-hour. As a result, 8 of the original 45 patients were eliminated from the study, and 24-hour ABPM data from 37 of the 45 patients were used in this study.
The 24-hour mean values of blood pressure and HR obtained by 24-hour ABPM are shown in Table 2. The 24-hour mean SBP, and DBP dropped from 152.0±14.7 to 142.7±13.9 mm Hg (p<0.01) and from 90.9±10.9 to 85.9±9.6 mm Hg (p<0.01), respectively. The 24-hour mean HR dropped from 72.9±6.5 to 67.4±6.6/min (n=37, p<0.01). In dipper-type hypertension cases (n=32), the 24-hour mean SBP and DBP dropped from 151.0±14.1 to 142.6±14.3 mm Hg (p<0.01) and from 90.6±10.2 to 86.3±9.5 mm Hg (p<0.01), respectively. The 24-hour mean values of HR were reduced slightly in dipper cases, but in non-dipper-type hypertension cases (n=5) these were significantly reduced from 77.1±9.6 to 65.5±9.4/min (p<0.05).
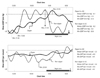
In order to assess the actions of efonidipine on the 24-hour SBP and HR, the average SBP and HR during a 24-hour period were plotted every 30 minutes throughout the day for patients whose mean SBP during the 24-hour period fell by 5 mm Hg or more after treatment with the drug (n=29) (Fig. 1A). The average diurnal SBP (7:00 a.m. to 10:00 p.m.) dropped significantly (p<0.05 or less), and average nocturnal SBP (10:30 p.m. to 6:30 a.m.) dropped slightly. Diurnal average HR decreased slightly, but no changes were seen in nocturnal average HR. Similarly, the average SBP and HR for subjects whose mean 24-hour SBP did not fall after treatment with the drug (n=8) are illustrated in Fig. 1B. In contrast to Fig. 1A, this graph shows that the average diurnal SBP after treatment was tended to be higher than that prior to treatment with the drug, and the average HR slightly decreased throughout the day. Three of these 8 patients were coincidentally under increased stress due to a busier work schedule than usual or due to a period of sleeplessness at the time of the second 24-hour ABPM that proved out the documentations of their diary during the examination consequently, their SBP values were unexpectedly elevated. These patients were followed without a change in the drug regimen. The remaining 5 patients were treated with efonidipine plus either an α, β-blocker (carvedilol; 5-10 mg/day) or an angiotensin II receptor blocker (candesartan; 8 mg/day). The 24-hour SBPs of all 37 patients were normalized after approximately 6 months.
Changes in the mean diurnal SBP (7:00 a.m. to 10:00 p.m.) and the mean nocturnal SBP (10:30 p.m. to 6:30 a.m.) are illustrated in Fig. 2. The mean diurnal SBP decreased from 165.0±12.4 to 145.2±13.5 mm Hg after treatment with the drug in the dipper cases (p<0.05) as show in upper left graphs. In the non-dipper cases, mean nocturnal SBPs dropped significantly from 159.1±15.5 to 137.3±19.2 mm Hg (p<0.01) as show in upper right graphs. The D/N SBP ratios in both groups are illustrated in the lower graphs. The D/N SBP ratio reduced from 16.7±6.1% to 8.3±9.8% in dipper cases (p<0.05), and increased from 2.3±2.9% to 7.7±5.1% in non-dipper cases (p<0.01), because the SBP drop was more marked during nighttime in the latter group.
To perform more accurate assessments of the antihypertensive actions of the drug, ΔSBP and ΔHR were measured in each patient at 30-minute intervals during the 24-hour period before and after treatment with the drug. After obtaining the average ΔSBP and ΔHR every 30 minutes in dipper and non-dipper cases, their best-fit curves were generated using MEM-LSM. Fig. 3 shows the best-fit curves of the average ΔSBP and ΔHR, which indicate the antihypertensive effect of the drug throughout the day. The average administration time of the drug after waking was 6:30 a.m., as indicated by the thick arrows. This figure shows the superimposed curves of the average 24-hour ΔSBP and ΔHR in both dipper and non-dipper cases. As shown in the upper graph of this figure, the median values of the periodic function for the average 24-hour ΔSBP (MESOR) were -9.1 mm Hg in dipper cases and -9.2 mm Hg in non-dipper cases. In the dipper cases, the antihypertensive effect was maximized at 11:30 a.m., 5.0-hour after administration of the drug. During this time, the mean drop in SBP was 4.7 mm Hg/h. The antihypertensive effect showed maximum attenuation at 12:30 a.m., 19.0 hours after administration of the drug, during which the mean rise in SBP was 2.1 mm Hg/h. The non-dipper cases showed ΔSBP changes opposite to those seen in dipper cases from noon to night-time. The rise in SBP in the morning was suppressed in both dipper and non-dipper cases. The lower graph of Fig. 3 illustrates the changes in the average 24-hour ΔHR before and after treatment with the drug. Median 24-hour ΔHR was -2.3/min in dipper cases, and -5.4/min in non-dipper cases. In the dipper cases, a continuous reduction in ΔHR was seen from 3.5 to 23 hours after administration of the drug. In the non-dipper cases, ΔHR values were unstable and showed a decrease from day-time to midnight, but were elevated after waking (6:30 a.m.). The change in ΔHR seemed to occur without correlation to the passage of time from the administration of the drug.
Discussion
In this study, best-fit curves were used to analyze circadian changes in ΔSBP and ΔHR before and after efonidipine monotherapy upon awakening. As demonstrated in Fig. 3, maximum antihypertensive action was observed at 5 hours after the morning dosing, and this action was long-lasting with a duration of 11-12 hours. In a pharmacokinetic study in humans, the Tmax and Cmax of efonidipine were 2.5±0.3 hours, and 19.0±6.0 ng/mL, respectively.18) The biliary system was the main route of elimination for this drug.18) In experiments with spontaneously hypertensive rats, the hypotensive action of NZ-105 (efonidipine; 5 mg/kg) peaked at 3 hours and lasted for more than 9 hours, while that of nicardipine (5 mg/kg) peaked at 0.5 hours and lasted for 3 hours.11) A pharmacodynamic study showed that the binding affinity of 3H-efonidipine for DHP receptors in rabbit aortic microsomes was 5.7-fold less potent than that of 3H-nitrendipine, and the dissociation constant (Kd) of 3H-efonidipine (4.48 nM) was approximately 6 times larger than that of 3H-nitrendipine (0.79 nM).19) On the basis of these experimental results, efonidipine has been considered to belong to the group of slow-onset and long-lasting CCB. In the present study, efonidipine did not fully demonstrate the typical characteristics of long-lasting CCBs, an effect that may be attributed to a major difference in its dosing: 5 mg/kg in experiments vs. 40 mg once daily in clinical medication. The hypotensive action of efonidipine peaked at 5 hours after administration. The rate of the drug's hypotensive effect was 4.7 mm Hg/h, and it slowly recovered at a constant rate (2.1 mm Hg/h) over 12 hours in dipper cases, which appears to be a characteristic property of efonidipine. The D/N SBP ratio significantly decreased (from 16.7±6.1% to 8.3±9.8%) after treatment with efonidipine, chiefly due to the fall in diurnal SBP in dipper cases. In previous studies, a once-daily morning dose of typical long-lasting CCBs (amlodipine, nifedipine GITS, nisoldipine ER, etc.) was shown to be equally effective in reducing the mean 24-hour SBP level. The D/N SBP ratios before and after treatment were 11.2% and 11.0% for nifedipine GITS, and 5.1% and 5.7% for amoldipine.20)21) Thus, the hypotensive effect of efonidipine on nocturnal SBP reduction in dipper cases was weaker than that of typical long-lasting drugs. On the other hand, an interesting hypotensive effect of efonidipine that was not time-dependent was observed in non-dipper cases; however, this result was not conclusive due to the small number of cases. Further study consisting of a larger sample size is needed to better understand these phenomena.
The MorBidity-mortality EvAIUaTion of the If inhibitor ivabradine in patients with coronary disease and left ventricULar dysfunction (BEAUTIFUL) study demonstrated that elevated HR is associated with an increased risk of cardiovascular mortality.22) The mean reduction in 24-hour HR after treatment with a long-lasting CCB in previous studies was smaller than that observed in this study, and in most studies it did not significantly change, even when a long-lasting L- and N-type CCB was administered.14) A recent study demonstrated that resting HR decreased significantly after treatment with efonidipine.23) In the present results, the mean 24-hour HRs decreased significantly (p<0.01). A well-known disadvantage of the hypotensive effect of L-type CCBs is that it is accompanied by reflex tachycardia.22) Previous studies have noted that the hypotensive effect of efonidipine is accompanied by less or no reflex tachycardia.24) The direct suppression of phase 4 depolarization (pace-maker potential) in the sinus node, which is produced by the blockage of these channels, is likely to be a cause of the decrease in 24-hour HR.12) The slow, constant recovery of SBP after the initial drop may also contribute to HR reduction. These properties of efonidipine may be related to the present results, in that the changes in ΔHR during 24 hours were not dependent on administration-time.
In summary, the antihypertensive actions of efonidipine were characterized by an administration time-dependent fall in 24-hour SBP (4.7 mm Hg/h) and a long-lasting recovery of the decrease in SBP at a constant rate (2.1 mm Hg/h), in addition to a non-administration time-dependent decrease in 24-hour HR. To understand the precise action of L- and T-type CCB, further clinical studies will be needed.
 : average systolic blood pressure before drug administration,
: average systolic blood pressure before drug administration,  : average systolic blood pressure after drug administration,
: average systolic blood pressure after drug administration,  : average heart rate before drug administration,
: average heart rate before drug administration,  : average heart rate after drug administration. Each value represents an average value±SD. *p<0.05, †p<0.01.
: average heart rate after drug administration. Each value represents an average value±SD. *p<0.05, †p<0.01.



 XML Download
XML Download