

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Complete fracture, migration, dislodgement, or entrapment of large bore guide wires such as 0.035 or 0.038-inch wires during percutaneous coronary intervention (PCI) or percutaneous transluminal angioplasty (PTA) for peripheral arterial disease is a very rare event. The guide wire remnants could lead to complications such as thrombosis, embolic phenomena, or vessel occlusion.1-3) Most reports regarding guide wire fractures have demonstrated fracture of guide wires in the coronary arteries;1-6) however, guide wire fractures in the peripheral arteries are seldom reported.7) We observed a 0.035-inch Terumo wire fracture and dislodgement of the guide wire in the femoral artery during PCI. After failure of the commonly used retrieval method by snaring, the retained wire fragment was successfully retrieved using a biopsy forcep, which was originally designed for myocardial biopsy. We report this case as an effective novel retrieval method in cases of an unexpected fracture and dislodgement of a larger profile wire.
Case
An 85-year-old man presented with crescendo chest pain that did not respond to nitroglycerin. He had suffered from hypertension, chronic kidney disease, and had a 7-year history of chronic stable angina pectoris.
Coronary angiography through the right radial artery was performed. The angiographic findings showed total occlusion (thrombolysis in myocardial infarction grade 0) in the left circumflex (LCX) artery, and the right coronary artery (RCA), and 75% severe stenosis in the left anterior descending artery (LAD). The collaterals were filled from the LAD to the RCA (grade 2) and LCX (grade 1). PCI was not performed because of the patient's age and chronic kidney disease state. After intensive medical treatment including antiplatelet agents, antianginal agents, antihypertensives, and a statin, the patient's ischemic symptoms improved. He was discharged for regular clinical follow-up at the outpatient department.
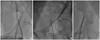
Six months after the index discharge, the patient returned to the emergency department with acute ischemic chest pain and was diagnosed with a non ST-segment elevation myocardial infarction (NSTEMI). Early invasive management strategy was decided, and he was transferred to the cardiac catheterization laboratory for emergent angiography and subsequent PCI. The left femoral artery was punctured for vascular access and a guide wire, so-called 035 Terumo wire (0.035 Radiofocus® Guidewire M, Terumo Corp., Somerset, NJ, USA), was inserted with a 5 Fr diagnostic angiography catheter but it did not pass well through the stenotic external iliac artery, which was found incidentally. Iliofemoral angiography through the femoral sheath showed a tortuous external iliac artery with significant focal stenosis (Fig. 1A). While inserting the 035 Terumo wire through the focal iliac stenotic lesion, the wire tip became kinked and was trapped in the lesion. Attempts to remove the wire caused unraveling of the coiled tipped structure, followed by complete fracture, leaving a long thin filament in the proximal femoral and distal external iliac artery.
Multiple attempts to retrieve the wire percutaneously using an Amplatz GooseNeck snare (EV3, Plymouth, MN, USA) were unsuccessful (Fig. 1B), and the fractured wire migrated to the superficial femoral artery. A 5 Fr multipurpose catheter was used to push the migrated fractured wire from the femoral sheath to the external iliac artery for retrieval by the snare device, but that attempt also failed (Fig. 1C).
Another ipsilateral anterograde femoral puncture was performed to approach from the upper side of the entrapped wire at a higher level than the femoral artery. Retrieval was attempted again with the Amplatz GooseNeck snare but was unsuccessful.
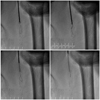
After these methods failed, a cardiac biopsy forcep (5.5 Fr, 104 cm, Cordis, Bridgewater, NJ, USA), which is commonly used for myocardial biopsy, was inserted through a transport catheter. After multiple forward and backward movements of the forcep, the fractured guide wire was successfully grabbed and finally retrieved (Fig. 2).
Immediately after removing the fractured and entrapped guide wire, PCI was successfully performed through the right femoral artery for the LAD culprit lesion, and the patient was safely discharged for clinical follow up.
Discussion
Guide wire fractures during PCI are very rare, occurring in approximately 0.1-0.2% of all cases. Furthermore, fracture, migration, and entrapment of 0.035-inch large diameter wire is extremely rare. Some reports have considered removal techniques for fractured guide wires in the coronary artery.2)4)8) These guide wires were always the 0.014-inch usual coronary guide wires, but this is the first report regarding successful retrieval of a fractured 0.035-inch guide wire.
Radiofocus Guidewire, so-called 035 Terumo wire, is commonly used during PCI to place the diagnostic or guiding catheter via a transradial or transfemoral route. The present case demonstrates that if a guide wire enters a severely stenotic peripheral artery, the wire may get trapped, so caution should be exercised to prevent this situation. Once the distal tip becomes wedged, forceful pulling on the wire may lead to fracture. Our case was unique in that the fractured guided wire was 0.035 Radiofocus Guidewire, and the fracture and migration occurred in the peripheral artery. The guide wire remnants theoretically could lead to complications, such as thrombosis, embolic phenomena, vessel occlusion, or associated limb ischemia. Therefore, patients should be referred for surgical intervention in the event of a failed percutaneous retrieval and subsequent persistent signs of ischemia.
There are several methods recommended for managing fractured guide wires in arteries, including emergent surgery,3) loop snare removal,5) use of an embolic protection device,4) stenting over the retained wire,5) and conservative treatment.6) We considered these methods for our case to successfully retrieve the fractured and remaining 035 Terumo wire in the femoral artery.
Attempts to remove a fractured wire using a peripheral snare were unsuccessful. It could be partially explained by the fact that because a 0.035 Terumo wire is thicker than a 0.014-inch wire, the direction of removing the fractured wire was against the blood flow via the femoral sheath, and floating and moving of the wire fragment could not be controlled retrogradely without any device for grabbing. If we had tried again from the contralateral femoral artery with a large bore guiding sheath and attempted to grab with a snare device, we may have successfully retrieved the wire, because a snare device can be controlled more effectively. However, in this situation, we have to was bigger contralateral guiding sheath and this will requre another percutaneous closure device in the contralateral femoral access site after the procedure, which is a less cost-effective method.
Surgical treatment should be considered after failure of commonly used techniques. However in this case with NSTEMI, surgical procedures could delay the PCI time, so a surgical option was considered inappropriate. Instead, we used a cardiac biopsy forcep, which is commonly used in the cardiac catheterization laboratory for a myocardial biopsy, and finally the fractured guide wire was successfully retrieved via an ipsilateral anterograde approach.
Our case highlights a new technique to help successful retrieval of a retained 035 wire in a peripheral artery percutaneously during PCI or PTA. Cardiac biopsy forceps can be an useful option after snaring attempts are unsuccessful.
 XML Download
XML Download