

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Implantable cardioverter defibrillator (ICD) therapy has been shown to reduce the risk of sudden cardiac death (SCD) and improve survival in severe heart failure.1-3) The Multicenter Automatic Defibrillator Implantation Trial II (MADIT-II) showed a benefit of ICD therapy in patients with prior myocardial infarction (MI) and advanced left ventricular dysfunction.4)5) The Defibrillators in the Non-ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) trial reported that ICD reduced the risk of SCD from arrhythmia in severe, non-ischemic cardiomyopathy (NICMP).6) Based on these trials, the American College of Cardiology/American Heart Association/Heart Rhythm Society has recommended prophylactic ICD implantation as the primary intervention to prevent SCD in patients with severe heart failure.7)
Although Asian populations are known to have lower risks of SCD compared to Caucasians, there is a paucity of data on whether prophylactic ICD therapy has a beneficial effect on preventing SCD in Asian populations with heart failure.8) Japanese patients who met the MADIT-II criteria showed better survival rates than those of the MADIT-II conventional therapy group.9) Recently, Chinese patients with the same inclusion criteria as MADIT-II showed a similar cumulative probability of SCD to that of the MADIT-II conventional therapy group.10) However, there are few studies reporting the prognosis of NICMP in an Asian population. Therefore, the aims of this study were to investigate the clinical outcome of Korean patients with severe heart failure and who were candidates for ICD implantation as a primary prevention against SCD, and to compare those results with data from the conventional therapy groups in the previous MADIT-II and DEFINITE trials.
Subjects and Methods
Study population
A group of 588 consecutive patients who had ≤30% of left ventricular ejection fraction (LVEF) on echocardiography at Seoul National University Hospital from January 2003 to December 2006 were retrospectively enrolled. The cause of cardiomyopathy was evaluated and classified as follows: ischemic cardiomyopathy (ICMP) was defined as left ventricular dysfunction associated with coronary artery disease (>50% narrowing of the diameter of at least one of the 3 major coronary arteries on coronary angiography), a history of a MI, a regional wall motion abnormality in the echocardiography, abnormal perfusion in single photon emission computerized tomography, or a Q wave in the electrocardiogram.11) NICMP was defined as left ventricular dysfunction without a definite cause by coronary lesion.11) In patients with acute MI, echocardiography data were used, which was measured at least 40 days after MI. Only those with NICMP and whose LV systolic function was ≤30% after 3 months of medical therapy were included. Patients excluded from the study included those who did not have LVEF data after stabilization or had not been followed-up in an outpatient clinic for at least 3 months after appropriate medical therapy (n=81), those with an improved LVEF of >30% after medical therapy or a transient heart failure state due to uncontrolled tachyarrhythmia, sepsis, drug or other causes (n=171), and those who expired before discharge (n=54). Two patients with New York Heart Association (NYHA) functional class (Fc) I and 1 patient with a previously inserted ICD were excluded, and 4 patients who had undergone heart transplantation after severe heart failure were also excluded. Finally, 275 patients with severe left ventricular dysfunction with NYHA Fc II or III were enrolled. A cohort of 131 patients was classified as the ICMP group, and 144 patients were classified as the NICMP group. The institutional review board approved the study protocol.
Risk factor assessment
Basic demographic data were reviewed from the medical records. Data concerning atrial fibrillation (AF), hypertension, diabetes mellitus, chronic kidney disease, and valvular heart disease were syste-matically acquired. AF was diagnosed based on electrocardiography or a past medical history of AF treatment. Patients who had been previously diagnosed with hypertension and taken antihypertensive medicine were defined as hypertension patients. Patients with diabetes mellitus were defined as those who had been diagnosed by a fasting plasma glucose ≥126 mg/dL, plasma glucose ≥200 mg/dL 2 hours after taking 75 g of oral glucose, or symptoms of hyperglycemia and casual plasma glucose ≥200 mg/dL. Patients with a glomerular filtration rate <60 mL/min/1.73 m2 were diagnosed with chronic kidney disease. Patients with valvular heart disease were defined as those with stenotic valvular disease or valvular regurgitation at more than a moderate degree on the echocardiography. Information on prescribed medication which was used for >3 months during the follow-up period such as beta-blockers, angiotensin-converting-enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARB), amiodarone, digitalis, HMG-CoA reductase inhibitors, loop diuretics, potassium sparing diuretics, thiazide, anti-platelet drugs, or anti-coagulation drugs was collected. Modes of revascularization methods were classified as percutaneous coronary intervention (PCI), coronary artery bypass surgery (CABG), both PCI and CABG, or thrombolysis therapy.
Clinical outcomes
Follow-up data were obtained from hospital records, by telephone contact with family members, and from death certificates obtained from the National Statistical Office (NSO). Deaths were categorized by their causes, including SCD, non-SCD, unclassified cardiac death, non-cardiac death, and death from unknown causes. For in-hospital deaths, SCD was assigned according to hospital records by an attending physician or by evidence of an arrhythmic event, such as ventricular tachycardia or ventricular fibrillation.12) For out-of-hospital deaths, we obtained follow-up data by telephone contact with family members. Patients who experienced SCD were defined as those who died suddenly and unexpectedly within 1 hour of cardiac symptoms in the absence of progressive cardiac deterioration, those who died unexpectedly in bed during sleep, and those who died unexpectedly within 24 hours after last being seen alive.5)12) We used the database of Korean Standard Classification of Diseases from the NSO to classify those who could not be identified by the above 2 methods. Unclassified cardiac death was defined as cases in which the clinical information was inadequate to classify the cardiac deaths as sudden or non-sudden. Patients were followed until December 2008.
Statistical analysis
Continuous variables were expressed as the mean±SD, whereas categorical variables were presented as absolute values and percentages. Student t-tests were used to analyze continuous variables and chi-square tests were used for categorical variables. The log-rank test was used to compare Kaplan-Meier survival curves, and the Cox proportional-hazards model was used to adjust for covariates and to estimate the hazard ratio (HR) for death and the corresponding 95% confidence interval (CI). Survival tables obtained from the Kaplan-Meier analysis were used to compare the ICMP group to the MADIT-II trial group and the NICMP group to the DEFINITE trial group.
A standard normal distribution was used to compare the survival rates or incidence of SCD and to analyze continuous variables, and the chi-square test was used to analyze categorical variables, such as baseline characteristics. A multinomial logistic regression model was used to analyze the relationship between improvement of LV systolic function and multiple factors. All reported p were 2-tailed. Statistical Package for the Social Sciences version 17.0 was used for all statistical analyses and p<0.05 was considered statistically significant.
Results
Clinical characteristics of the study population
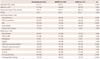
The baseline characteristics of both groups are presented in Table 1. The NICMP group was younger (56±14 vs. 65±11 years, p<0.001) and had more female patients than the ICMP group (42% vs. 29%, p=0.032). The NICMP group had a higher prevalence of AF and valvular heart disease than the ICMP group, whereas the ICMP group had more hypertension, diabetes mellitus, and renal disease. ICMP patients received HMG-CoA reductase inhibitors and anti-platelet therapy more frequently than the NICMP patients, whereas digitalis, thiazide and anti-coagulation therapy were prescribed more often in the NICMP group. Among 275 objective patients, 189 did not take any beta-blockers. Only 13% of these patients had contraindications such as chronic obstructive pulmonary disease or asthma (n=18, 10%), bradycardia or sick sinus syndrome (n=2, 1%), hypotension (n=2, 1%), or intolerance (n=2, 1%).
The ischemic cardiomyopathy group had a similar incidence of sudden cardiac death, but a higher all-cause mortality rate than the non-ischemic cardiomyopathy group
During the 40 months follow-up period, nearly one-third of the total population (80 patients, 29%) died from all causes of death. The causes of death in these 80 cases were obtained from hospital records (n=28), telephone contact with family members (n=18), or databases obtained from the NSO (n=34). SCD could be identified from in-hospital records (n=11), telephone contact with family members (n=10) and databases obtained from the NSO (n=2). Causes of death are summarized in Table 2. The all-cause mortality rate of the ICMP group was higher than that of the NICMP group (40% vs. 19%, p<0.001) (Fig. 1). However, there was no statistical difference in total cardiac death (21% vs. 15%, p=0.082), SCD (10% vs. 7%, p=0.272), non-SCD (5% vs. 3%, p=0.194), or unclassified cardiac death (6% vs. 5%, p=0.502) between the ICMP and NICMP groups. The ICMP group died of non-cardiac causes more frequently than the NICMP group (18% vs. 4%, p<0.001). There were 24 non-cardiac deaths in the ICMP group, including deaths from chronic renal failure with end-stage renal disease (n=8), complications of diabetes mellitus (n=5), systemic infection (n=3), malignancy (n=5), interstitial lung disease (n=1), cerebral infarction (n=1), and toxic hepatitis (n=1). In the NICMP group, non-cardiac deaths (n=6) were due to diabetic complications (n=3), chronic renal failure (n=1), and malignancy (n=2).
Ischemic cardiomyopathy and old age were independent predictors for all-cause death
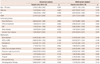
In a univariate analysis for all-cause death in the total population, old age {>70 years old, HR 2.16 (95% CI 1.37-3.39), p=0.001}, ICMP {HR 2.42 (1.52-3.85), p<0.001}, and potassium-sparing diuretics {HR 0.58 (0.36-0.93), p=0.025} were significant prognostic factors (Table 3). However, chronic kidney disease {HR 1.60 (0.99-2.59), p=0.053} and beta-blockers {HR 0.65 (0.39-1.08), p=0.080} did not show statistical significance as prognostic factors. In a multivariate Cox regression model, ICMP {HR 2.91 (1.52-5.59), p=0.001} and old age {>70 years old, HR 1.89 (1.13-3.15), p=0.015} were independent predictors for all-cause mortality. Valvular heart disease {HR 2.00 (0.93-4.33), p=0.078}, potassium-sparing diuretics {HR 0.59 (0.35-1.01), p=0.053}, and loop diuretics {HR 1.59 (0.97-2.61), p=0.069} were likely to be prognostic factors for all-cause mortality. There were no independent predictors for SCD (Table 4).
Ischemic cardiomyopathy {HR 6.18 (1.89-20.24), p=0.003}, chronic kidney disease {HR 2.80 (1.13-6.94), p=0.026}, HMG-CoA reductase inhibitors {HR 0.29 (0.11-0.76), p=0.012}, and digitalis {HR 2.05 (1.01-4.17), p=0.047} were independent predictors for non-cardiac death.
Subgroup analysis for cause of death
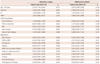
A univariate analysis of the ICMP group showed that anti-platelet medication, valvular heart disease, and digitalis showed statistical significance for all-cause death (p=0.036, p=0.023, and p=0.042, respectively). In a multivariate Cox regression analysis of the ICMP group, old age {>70 years old, HR 2.27 (1.15-4.47), p=0.018}, anti-platelet medication {HR 0.41 (0.18-0.92), p=0.030}, and revascularization therapy {HR 2.23 (1.05-4.73), p=0.036} were independent prognostic factors for all-cause mortality (Table 5). However, revascularization therapy was not a significant predictor for other causes of death, such as total cardiac death, SCD, non-SCD, or non-cardiac death. In 82 patients with revascularization therapy, 45 patients had undergone PCI therapy, 25 patients in the CABG and 10 patients in both the PCI and CABG, and 2 patients in thrombolysis. According to the method used for revascularization therapy, there was no method which showed statistical significance related to all-caused death.
The ICMP group was subdivided according to specified anti-platelet drugs: no anti-platelet drug (n=18, 14%), aspirin alone (n=62, 47%), clopidogrel alone (n=7, 5%), aspirin and clopidogrel (n=42, 32%), aspirin and cilostazol (n=1, 1%), and triple anti-platelet medication (aspirin, clopidogrel, and cilostazol, n=1, 1%). In a Kaplan-Meier pair-wise comparison according to the anti-platelet medication, patients with single or multiple anti-platelet medication showed better survival than those without anti-platelet medication, but this finding was not statistically significant (p=0.051 and p=0.057, respectively). However, there was no significant difference in prognosis between use of a single drug and use of multiple drugs (p=0.830). There was no independent predictor for SCD in the ICMP group. For non-cardiac death, chronic kidney disease {HR 4.29 (1.53-11.97), p=0.006} and HMG-CoA reductase inhibitors {HR 0.25 (0.08-0.85), p=0.025} were independent predictors.
In the NICMP group, valvular heart disease {HR 4.92 (1.47-16.51), p=0.010} and potassium sparing diuretics {HR 0.31 (0.11-0.86), p=0.025} were prognostic factors of all-cause mortality; however, there were no independent prognostic factors for SCD.
Improvement of left ventricular systolic function during follow-up period
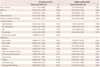
During the follow-up, 237 patients (131 patients in the NICMP group) had undergone follow-up echocardiography evaluation. Mean LVEF during follow-up was 28±8%. There was no significant difference in the change of LVEF during follow-up in both the NICMP and the ICMP group (5±9% vs. 5±7%, p=0.670). Ninety-two (39%) patients showed improvement in LV systolic function compared to baseline (the change in LVEF: 65±41%, absolute change: 13±6%). The number of patients in the NICMP group who had >25% improvement in LVEF was greater than the number in the ICMP group, but the difference was not statistically significant (42% vs. 35%, p=0.286). Patient characteristics were analyzed to identify those who showed improvement of >25% in LV systolic function compared to the baseline (Table 6). The improved group had a lower EF at baseline (22±5% vs. 25±4%, p<0.001) and took anti-platelet medication less frequently (51% vs. 66%, p=0.029).
Other baseline characteristics such as ischemic cause, medication, and other comorbidities were similar. Despite improvement of LV systolic dysfunction, there was no significant difference in clinical outcomes, i.e. all-cause mortality, SCD, total cardiac death, or non-cardiac death according to LV systolic improvement (all p>0.05).
Comparison of survival with Western population studies
To test whether the survival of the Korean population with severe heart failure was different from that of the Western population with heart failure, the clinical outcomes were compared with 2 well-known Western heart failure studies.5)6) The ICMP group was compared to the MADIT-II conventional group (n=490). There were no significant differences in age and mean LVEF, whereas the Korean ICMP group had fewer male patients (71% vs. 85%, p=0.001). In addition, beta-blockers (32% vs. 70%, p<0.001) and HMG-CoA reductase inhibitors (51% vs. 64%, p=0.006) were prescribed less often in the Korean ICMP group, and ACEI or ARB were prescribed more frequently (89% vs. 72%, p<0.001). In the 2-year mortality ob-tained from the Kaplan-Meier analysis, the ICMP group had a similar all-cause mortality (20% vs. 20%) and incidence of SCD (7% vs. 10%) compared to the MADIT-II conventional therapy group (respectively, all p>0.05) (Fig. 2).
The NICMP group was compared to the DEFINITE standard therapy group (no ICD, n=229). There was no significant difference in age and mean LVEF compared to the DEFINITE standard therapy group, whereas the percentage of males in the NICMP group was less than that of the DEFINITE standard therapy group (58% vs. 70%, p=0.026), and AF in the NICMP group was more frequent (43% vs. 26%, p=0.001). Beta-blockers (29% vs. 84%, p<0.001) were prescribed less in the Korean NICMP group. The probability of survival and SCD were similar in the Korean NICMP group and the DEFINITE standard therapy group (13% vs. 17%; 6% vs. 6%, all p>0.05) (Fig. 3).
Discussion
The present study showed several findings as follows: 1) ICMP patients had a poorer prognosis than NICMP patients, despite similar LV systolic dysfunction; 2) the incidence of SCD was similar in both groups; and 3) both ICMP and NICMP groups had comparable risks of SCD; similar to results in previous Western population studies.
Prognosis of Korean heart failure population
The mortality rate in our study population was 15% for 2 years and 29% for 40 months of follow-up. SCD accounted for nearly 33% of total deaths. When compared with previous studies, the mortality rate in our study was similar to the previous ones.13) Patients in previous studies, including those who were admitted for heart failure, had a 2-year cumulative survival rate of 80.1%.13) In addition, Chinese patients with MADIT-II criteria had an all-cause death rate of 26%, with a mean of 35 months for a follow-up period.10) The all-cause mortality rate for the control group in the MADIT-II study was 20% during 20 months follow-up.4) However, Japanese patients with similar MADIT-II criteria had a lower mortality rate than in previous reports and our results, and they reported a rate of 17% for death events, with an average of 37 months for the follow-up period.9) The Japanese paper reported a lower rate for SCD than the previous Chinese paper, MADIT-II, and our study.5)9)10) These differences could be explained by the difference in preval-ence of the patients with NYHA Fc I. Our study included only those patients with NYHA Fc II or III, whereas the Japanese study consisted of 79% NYHA Fc I patients.9) In addition, the Chinese study and MADIT-II study included fewer patients who were NYHA Fc I patients (27% and 39%, respectively).4)5)10) Advanced NYHA Fc might be an important risk factor for SCD in this population.14)15) Based on these results, we should be careful to recommend prophylactic ICD implantation in those patients with good functional status.
In comparison to the MADIT-II and DEFINITE studies, the number of prescriptions for beta-blockers was lower in our study. Although 13% of patients had contraindications for beta-blocker therapy, there is a need to investigate the exact reason why a beta-blocker was not prescribed in the retrospective study design. The Japanese heart failure study showed a prescription rate for beta-blockers similar to our study.9) Although we do not have statistical data on the prescription rate of beta-blockers in Korea between 2003 and 2006, there is one study that does address this question.16) The study fo-und that even tertiary hospitals prescribed beta-blockers for <20% of patients with heart failure and for 30% of patients with ischemic heart disease. Considering that our study included heart failure patients between 2003 and 2006, the prescription rate of beta-blockers might be lower than that in current practice, but not so different from other hospitals in a similar period. The Study of HF Awareness and Perception in Europe (SHAPE), which was performed in the early 2000s, analyzed the low prescription pattern of beta-blockers for heart failure patients in the real world.17) According to the SHAPE study, in mild to moderate stable HF patients without signs of fluid retention, only 25% of cardiologists started a beta-blocker with ACEI. Few cardiologists started therapy by using a beta-blocker only. Although there was no contraindication to beta-blocker therapy, elderly patients or those with ACEI or on diuretic therapy were less likely to receive a beta-blocker. Considering the high prescription rates for ACEI or ARB in our study, additional beta-blocker therapy might not be considered for stable heart failure patients. In our study, beta-blockers were not a statistically significant prognostic factor for all-cause mortality, SCD, or non-cardiac death, but the results were close to being significant {HR 0.65 (0.39-1.08), p=0.097}. Updated prescription rates for beta-blockers and their prognostic effect in a Korean heart failure population should be evaluated in a future study.
Similar criteria for prophylactic implantable cardioverter defibrillator implantation in both ischemic cardiomyopathy and non-ischemic cardiomyopathy
In this study, the mortality rate of the ICMP group was higher than that of the NICMP group. One of the explanations could be the difference in baseline characteristics. The ICMP group was older and frequently had more co-morbidities such as renal failure, hypertension, and diabetes, which are important prognostic factors. Diabetes and chronic kidney disease are well known to be poor prognostic factors of heart failure and risk factors for ischemic heart disease.18-21) HMG-CoA reductase inhibitors are known to reduce mortality among patients with severe heart failure and to lower the mortality in patients with hemodialysis.22)23) In a Cox regression analysis for non-cardiac death, chronic kidney disease was associated with a poor prognosis, whereas HMG-CoA reductase inhibitors were found to be related to a reduced risk of mortality. Therefore, a higher prevalence of comorbidities could increase the risk of non-cardiac death, which could be an important reason for the increased all-cause mortality in the ICMP group. Previous studies reported a difference in survival between NICMP and ICMP patients.11) Although NICMP patients were younger, patients with ICMP had poorer clinical outcomes than the NICMP patients.11)13) NICMP patients showed a greater improvement in symptoms and left ventricular function during follow-up.11) We found that the NICMP group was more likely to show improvement in LV systolic function than the ICMP group during follow-up, even though the difference was not statistically significant. Also, the improvement of LV systolic function was not a prognostic factor for all-cause mortality, SCD, or non-cardiac death.
The risk of SCD in our study group was not lower than in previous Western population studies. Therefore, the current guidelines for prophylactic ICD implantation based on Western populations are acceptable in Korean patients with heart failure.
In conclusion, the risk of SCD in Korean patients with severe heart failure and fulfill the prophylactic ICD implantation criteria is comparable to those of other Asian studies and Western population studies. This suggests that prophylactic ICD implantation in this population might provide a beneficial effect similar to that found in other Asian and Western populations.
Study limitations
This study was conducted at a single tertiary center and was a retrospective study, so there is a limitation when extrapolating these results to the entire Korean population. For those who died out-of-hospital, the cause of death was classified based on the death certificates and telephone contact with family members. There might be a possibility that some SCD events could have been misclassified as non-SCD or non-cardiac death, which could underestimate the SCD risk in this population. Also, there could be recall bias of family members. The study population was smaller than the study populations in the MADIT-II and DEFINITE studies. However, considering the similar reports from other Asian countries, the number of subjects in our study was comparable. The prescriptions for beta-blockers and HMG-CoA reductase inhibitors were less than in previous reports, such as MADIT-II and DEFINITE.5)6) However, the prescription of beta-blockers was not lower than the average prescription rate in Korean patients with heart failure.16) We used the inclusion criteria described in the Korean medical reimbursement guideline; therefore, the conventional group in the DEFINITE trial had less severe inclusion criteria than our NICMP group. However, there is no large-scale trial which had the same inclusion criteria as our study. Although the conventional group in the DEFINITE trial included those with 31-36% of LVEF, there was no significant difference in the mean LVEF compared to our NICMP group. In addition, the clinical outcome was similar in the 2 groups.




 XML Download
XML Download