

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Thrombospondin 1 (TSP-1) was initially discovered in platelets as a thrombin-sensitive protein1) and is a matricellular protein that regulates cell-cell and cell-matrix interactions.2)3) Functional studies in TSP-1-/- mice have shown that TSP-1 inhibits angiogenesis,4) promotes the healing of excision wounds,5) and limits inflammatory responses and fibrotic remodeling after myocardial infarction.6)
TSP-1 also plays a role in platelet aggregation and thrombus adhesion to injured blood vessels and limits nitric oxide-mediated vasodilatation and tissue perfusion in experimental models of ischemic injury.7)
Thrombospondin-1 may represent a link between diabetes mellitus (DM) and vascular complications.8)9) High levels of glucose increase TSP-1 expression in renal mesangial cells.10) TSP-1 promotes the pathological events associated with diabetic nephropathy such as mesangial cell proliferation and increased extracellular matrix production by mesangial cells.10-13) A peptide blocking the activation of transforming growth factor-β by TSP-1 prevents the progression of cardiac fibrosis and improves cardiac function in a rat model, suggesting that TSP-1 plays an important role in the development of diabetic cardiomyopathy.14)
However, the precise role of TSP-1 in human atherosclerosis remains unknown. Therefore, the present clinical study was conducted to examine the association between TSP-1, coronary artery disease (CAD), and DM.
Subjects and Methods
Study patients
The study involved 374 consecutive subjects (206 men and 168 women) with suspected CAD from November 2008 to October 2009. Patients had undergone coronary angiography (CAG) to evaluate angina. The exclusion criteria included acute coronary syndrome, a serum creatinine level ≥2.0 mg/dL, and type 1 DM. This study was approved by our institutional review board. Each participant provided written informed consent prior to procedures being performed, and potential risks were fully explained.
Patients were considered to have DM if their fasting plasma glucose concentration was ≥126 mg/dL, or their two casual plasma glucose concentration was ≥200 mg/dL.15) Systemic hypertension was defined as a systolic blood pressure ≥140 mm Hg or a diastolic pressure ≥90 mm Hg.16) Smokers were defined as those who were currently smokers or who had a recent history of smoking (i.e., within the past 1 year). A family history of premature CAD was defined as CAD in a male first-degree relative <55 years old and a female first-degree relative <65 years old. Body mass index (BMI) was calculated using weight (kilograms) divided by the square of the height (meters).
Coronary angiography
Coronary angiography was performed with fasted patients using the Judkins technique. Stenosis severity was determined by visual estimation in two orthogonal views. Angiographic films were interpreted by angiographers without knowledge of patient laboratory data. Significant coronary stenosis was defined as a stenosis >50% in the left main trunk or >70% in the other major epicardial coronary arteries. Patients with CAD were defined as patients with at least one significant coronary stenosis.
The angiographic characteristics of the coronary atherosclerotic lesions were defined using Gensini's score.17) In this scoring system, a greater reduction in the luminal diameter receives a high score and a proximal lesion in the left anterior descending or the left circumflex artery is assigned a higher score than that of a distal lesion.
Laboratory analysis
Blood was sampled on admission to measure blood chemistry. For lipid profiles, patients fasted overnight and blood samples were obtained by venipuncture. Total cholesterol (TC), triglyceride (TG), high density lipoprotein-cholesterol (HDL-C), low density lipoprotein-cholesterol, and high sensitive C-reactive protein (hs-CRP) concentrations were determined using standard biochemical procedures on a Toshiba automated clinical chemistry analyzer (Toshiba, Tokyo, Japan). The glycated hemoglobin (HbA1c) level indicates the mean blood glucose level during the previous 2 to 3 months. HbA1c concentrations were measured using a commercially available glycohemoglobin analyzer (Tosho, Tokyo, Japan).
After an overnight fast, blood samples for TSP-1 were drawn at the time of CAG, before administration of contrast agent or medications. Samples were centrifuged to obtain plasma, and the plasma was immediately stored at -70℃ for subsequent analysis. Plasma TSP-1 concentration was assessed using a TSP-1 ELISA kit (R&D Systems, Minneapolis, MN, USA) that had a minimum detection level of 0.355 ng/mL.
Statistical analysis
Categorical variable data are expressed as numbers and percentages of patients. Continuous variable data are expressed as mean±SD. A one-way analysis of variance was used to compare the variables shown in Table 1 and Fig. 1. Post hoc comparisons between different groups were conducted with Scheffe's multiple comparison procedures. Chi-square tests were used for categorical variables. Pearson's correlation coefficient analysis was used to assess the association between measured parameters. Multivariate logistic regression analysis was used to identify CAD predictors. Univariate variables with a p<0.20 were entered into multivariate logistic models. Multivariate adjusted odds ratios (ORs) are shown with 95% confidence intervals (CIs). Differences were considered significant at p<0.05.
Results
Baseline patient characteristics
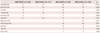
The clinical characteristics of patients in each group are shown in Table 1. The four groups were not similar in terms of age, gender ratio, hypertension, family history of CAD, BMI, serum creatinine, TG, HDL-C, hsCRP, or TSP-1 levels. Patients with CAD were older and had higher serum creatinine levels compared to patients without CAD, regardless of DM. Patients with DM and without CAD {DM(+)CAD (-) patients} had the highest BMI and TG levels. Patients without CAD had higher HDL-C levels compared to those in patients with CAD, regardless of DM. HsCRP was highest in patients with DM and CAD {DM(+)CAD(+) patients}. The incidences of male gender and a family history of CAD were highest in patients without DM and with CAD {DM(-)CAD(+)}, and the incidence of hypertension was higher in patients with DM than that in patients without DM. The four groups were similar in terms of smoking rate, TC, LDL-C, and uric acid. No statistical difference was observed between HbA1c level of DM(+)CAD(+) patients and that of DM(+)CAD(-) patients. When we divided patients with CAD based on DM, Gensini's score, and the number of involved vessels, no significant difference was observed between DM(+)CAD(+) patients and DM(-)CAD(+) patients.
Plasma thrombospondin-1 levels according to diabetes mellitus and coronary artery disease
Patients were divided into four groups to analyze plasma TSP-1 levels. We found that the plasma TSP-1 concentration was higher in DM(+)CAD(+) patients compared to that in patients without DM and without CAD {DM(-)CAD(-) patients}, DM(-)CAD(+) patients, and DM(+)CAD(-) patients (p<0.01) (Fig. 1A). When patients were divided into two groups according to DM, plasma TSP-1 levels were higher in patients with DM than those in patients without DM (564.5±113.5 ng/mL vs. 515.5±127.4 ng/mL, p<0.001) (Fig. 1B). When patients were divided into two groups based on the development of CAD, plasma levels of TSP-1 were not significantly different between the non-CAD and CAD group (Fig. 1C).
Baseline patient medications
Patient medications in each group are shown in Table 2. The four groups were not similar in angiotensin converting enzyme inhibitor/angiotensin receptor blocker (ACEi/ARB) or β-blocker use. The DM group had a higher rate of ACEi/ARB use than that in the non-DM group. The CAD group had a higher rate of β-blocker use than that in the non-CAD group.
In patients with DM, metformin was more frequently prescribed in the CAD group than that in the non-CAD group, and an α glucosidase inhibitor was more frequently prescribed in the non-CAD group than that in the CAD group.
Correlations between plasma thrombospondin-1 concentration and other variables
We examined whether TSP-1 levels correlated with any other various parameters or medications in all patients. We found no parameter or medication that correlated with TSP-1 concentration in any patient (Table 3).
Gensini's score was not correlated with plasma TSP-1 levels in CAD(+) patients (Pearson's coefficient=-0.047, p=0.489).
Logistic regression analysis
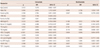
A simple logistic regression analysis showed that CAD was significantly correlated with gender, BMI, HDL-C, and plasma TSP-1 levels in patients with DM (Table 4). Simple logistic regression analysis variables with a p<0.20 were entered into a multivariate logistic model. The analysis revealed that male gender and HDL-C, HbA1c, and plasma TSP-1 levels were independently correlated with the development of CAD in patients with DM (OR, 2.728; 95% CI, 1.035-7.187; OR. 0.936; 95% CI, 0.894-0.979; OR, 1.373; 95% CI, 1.037-1.817; OR, 1.003; 95% CI, 1.000-1.007, respectively).
In non-DM patients, age, male gender, and family history were independent factors for CAD (OR, 1.043; 95% CI, 1.011-1.075; OR, 2.212; 95% CI, 1.159-4.222; OR, 3.350; 95% CI, 1.241-9.044, respectively).
Discussion
The present study is the first to show a link between human plasma TSP-1 concentrations and CAD in patients with DM. We found that plasma TSP-1 levels were higher in DM(+) CAD(+) patients than those in other patients, but that plasma TSP-1 levels were not different between CAD and non-CAD patients in patients without DM. A multivariate analysis showed that a high TSP-1 level was an independent predictor of CAD in patients with DM.
Vascular smooth muscle cell (VSMC) migration and proliferation are key events in the development of atherosclerotic lesions. VSMCs from patients with diabetes exhibit increased proliferation, adhesion, and migration. Stimulating VSMCs through increased levels of TSP-1 in the diabetic vessel wall may explain the enhanced proliferation of VSMCs.18)19) Two mechanisms have been suggested for the effect of higher plasma TSP-1 level on atherosclerosis in patients with DM.8) First, dysfunction of endothelial cells (ECs) in patients with DM is well known20) and TSP-1 certainly contributes to this dysfunction because of its antiproliferative and apoptotic effects on ECs.21)22) Second, although TSP-1 in diabetic vessels may affect metabolism of the luminal EC monolayer and VSMCs, the large amounts of TSP-1 present in the adventitia ultimately results in compromised growth and remodeling of the vasa vasorum. Indeed, a previous study showed that the number of vasa vasorum cells decrease in the diabetic aorta and are inversely correlated with TSP-1 expression, a potent antiangiogenic agent.8) In blood vessels, this may lead to ischemic conditions in the inner layers of the vessel wall, and such oxygen stress could stimulate VSMC proliferation and initiate atherosclerotic lesions.
Few studies of the effect of TSP-1 on CAD have been performed in humans. McGillicuddy et al.23) showed that fluvastatin decreases TSP-1 expression and abolishes the ability of transforming growth factor-β1 to induce TSP-1 expression in cultured human coronary artery smooth muscle cells. Recent studies have linked the TSP family, including TSP-1, to the development of atherosclerosis at the genetic level.24-26)
Glucose regulates the expression of a number of vascular genes.27) Activation of TSP-1 transcription is mediated by the glucose hexosamine pathway of catabolism, resulting in modulation of nuclear protein activity via glycosylation.9) In the present study, the TSP-1 level of DM(-)CAD(+) patients was not higher than that of DM(-) CAD(-) patients, suggesting that the release of TSP-1 is not related with CAD in patients without DM. We also found higher concentrations of human plasma TSP-1 in DM(+)CAD(+) patients compared to those in the other groups (Fig. 1A). However, we found that TSP-1 was not correlated with HbA1c. Gensini's score was not positively correlated with plasma TSP-1 level in patients with CAD, suggesting that a high TSP-1 level did not result in severe CAD.
Some differences in medication usage were observed, but Table 3 shows no correlation between medication use and plasma TSP-1 levels, suggesting that the differences in TSP-1 levels do not originate from medication differences.
A multivariate regression analysis of patients with DM showed that male gender, a low level of HDL-C, a high level of HbA1c, and a high level of plasma TSP-1 were independently and positively associated with CAD. Male gender and a low level of HDL-C are well known risk factors for cardiovascular events. In prospective epidemiological studies, the incidence of CAD is directly associated with the degree of hyperglycemia, as measured by HbA1c. After adjusting for other risk factors, an increase of 1% in the HbA1c level is associated with an 18% increased risk for cardiovascular events.28) We found that high HbA1c level was a risk factor for CAD, as previously reported.
Our findings suggest that high TSP-1 plasma levels may be associated with CAD in patients with DM. Although the physiological function of TSP-1 in humans is not fully understood, our cross-sectional data showed a positive correlation between plasma TSP-1 and the incidence of CAD in patients with DM. Long-term clinical follow-up with a larger group of patients with DM is required to confirm these findings.
Study limitations
The present study had some limitations. First, we enrolled a relatively small number of patients. Second, the study only included patients undergoing CAG, which may have biased the findings. Third, the prevalence of diabetes may have been underestimated, because a 75-g oral glucose tolerance test was not performed.
Conclusion
Plasma TSP-1 levels were higher in DM(+)CAD(+) patients than those in other patients. But, in the non-DM group, plasma TSP-1 levels showed no difference between patients with or without CAD. Plasma TSP-1 level was an independent predictor for CAD in patients with DM, indicating that increased plasma TSP-1 level might be associated with CAD in patients with DM.



 XML Download
XML Download