

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stents reduce clinical and angiographic restenosis compared to conventional balloon angioplasty.1) However, in a number of patients with implanted stents, neointimal hyperplasia produces in-stent restenosis (ISR).2) Although often considered a benign process, recent data reveals that ISR has a negative impact on long-term survival.3) In fact, repeated procedures have been associated with a higher risk of myocardial infarction and stent thrombosis.4) Vascular brachytherapy was the approved therapy, in comparison with balloon angioplasty,5)6) but recent studies suggest that drug-eluting stents (DES) may be superior to brachytherapy.7)8) We experienced one intractable ISR case which repeated regardless of successful brachytherapy treatment, and which was treated using DES.
Case
On February 2000, a 51-year-old man was admitted to the hospital with an acute anterior ST-segment elevation myocardial infarction. His electrocardiogram (ECG) showed ST-segment elevation in V1-5. After thrombolytic therapy using recombinant tissue plasminogen activator, stent implantation was performed from the proximal left anterior descending artery (LAD) to the mid LAD using 3.0×27 mm bare-metal stent (BMS) as an elective percutaneous coronary intervention (Fig. 1).
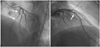
One year later, recurrent chest pain developed and an ECG showed ST-segment elevations in V1-5. Coronary angiography (CAG) revealed type IV (total) ISR in the proximal LAD, which was treated with balloon angioplasty using a 3.0×20 mm balloon (the first ISR). One year after that, recurrent chest pain developed, and ECG showed no ST-T changes, but CAG revealed type II (diffuse) ISR. This second ISR was treated with brachytherapy with a Rhenium filled balloon (300 seconds at 6 atm using a 3.0×20 mm balloon) (Fig. 2).
Four months later, recurrent chest pain developed once again and an ECG showed ST-segment elevations in V1-4. CAG revealed type IV ISR secondary to brachytherapy failure, which was treated with 3.0×20 mm balloon and 3.0×18 mm BMS implantation distal to the previously implanted BMS (the third ISR) (Fig. 3). Three months later, chest pain recurred and ECG showed ST-segment elevations in V3-5. CAG revealed type II ISR, which was treated with only ballooning (the fourth ISR). Nine months later, recurrent chest pain developed, and ECG showed no ST-T changes. CAG revealed type II ISR in the proximal and mid LAD stent. A 3.0×33 mm Cypher stent® (Cordis Johnson & Johnson, Bridgewater, NJ, USA) was implanted to treat this fifth ISR presentation (Fig. 4). The patient then remained asymptomatic and the 5-year follow-up CAG showed no ISR (Fig. 5).
Discussion
Bare-mental stent has improved procedural success and long-term outcomes, and reduced clinical and angiographic restenosis compared to plain old balloon angioplasty (POBA).1)9) Although stenting can resolve elastic recoil, negative remodeling and dissection caused by POBA and neointimal hyperplasia produces ISR in 20% to 50% of the patients implanted stent.2)10) ISR is often considered to be a benign process, but a recent report showed that it presents with acute myocardial infarction or unstable angina in over one-third of cases3) and has a negative impact on long-term survival.11) In fact, repeated procedures have been associated with a higher risk of myocardial infarction and stent thrombosis.4)
There are many treatment options for ISR. Although POBA is the first-line option, its results have been disappointing. Repeated use of BMS also exacerbates the risk of recurrence. Coronary artery bypass surgery may be an option for the treatment of recurrent ISR after BMS implantation. Alternative options, such as rotational atherectomy, excimer laser angioplasty, and cutting balloon did not reduce recurrent ISR.12)
Several reports show the efficacy of brachytherapy in patients with ISR,5)6)13)14) but brachytherapy presents problems such as logistical complexity, expense, and durability.12) Recent studies suggest that DES is superior to POBA,8)15) and moreover DES may even be superior to brachytherapy.7)8) This is a unique case for the successful management of intractable ISR with DES, even after POBA, BMS and brachytherapy.
In conclusion, we experienced an intractable ISR case, which can be treated by using DES. As recent studies show, DES is the best treatment option for ISR, and may even be used successfully to treat brachytherapy failure and intractable ISR.




 XML Download
XML Download