

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A family of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors known as statins reduce blood levels of low density lipoprotein-cholesterol (LDL-C) and form the cornerstone of treatment of hyperlipidemia to reduce cardiovascular morbidity and mortality.1-4) Low serum concentrations of high density lipoprotein-cholesterol (HDL-C) are one of the major risk factors for adverse events related to coronary atherosclerosis 5) and are highly prevalent among patients with acute coronary syndrome.6) A previous study showed that each 1 mg/dL increase in HDL-C is associated with a 2% to 4% reduction in coronary heart disease (CHD) outcomes.5) According to the National Cholesterol Education Program, low levels of HDL-C (<40 mg/dL) have been identified as a coronary risk factor within the guidelines for treatment of hyperlipidemia.7)
Niacin at pharmacologic doses reduces total cholesterol, triglycerides (TGs), very-low-density lipoprotein (VLDL), LDL-C, and lipoprotein(a) {Lp(a)}, and increases HDL-C levels.8)9) Of available lipid-regulating agents used to increase HDL levels, Niacin is the most potent. Several studies demonstrate that treatment with niacin, alone or in combination with other lipid-lowering agents, significantly reduces total mortality and coronary events, and retards the progression and induces regression of coronary atherosclerosis.8)9) The HDL Atherosclerosis Treatment Study (HATS) demonstrated that the combined use of niacin and simvastatin dramatically improved angiographic end points and led to a significant reduction in clinical cardiovascular events (>80% decrease) and significant coronary stenosis regression compared with placebo.10) The recent ARBITER 2 and 3 trials showed that extended-release niacin significantly increases HDL-C and induces regression of atherosclerosis measured by carotid intima-media thickness (CIMT) when added to statin therapy.11)12) But, there is little data that the combined effects of extended-release niacin and statin are synergistic in inducing regression of atherosclerosis measured by intravascular ultrasound (IVUS). Accordingly, the purpose of the present trial was to identify any synergy between niacin and simvastatin compared with simvastatin alone on plaque regression (measured by serial IVUS) and on inflammatory markers.
Subjects and Methods
Study population
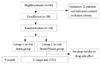
This study was a pilot, prospective, randomized and open-label study. It focused on coronary plaque regression in angina patients who had mild to moderate degree of coronary stenosis and who received niacin 1,000 mg plus simvastatin 40 mg or simvastatin 40 mg alone. The hypothesis of this study was that the combination of niacin and simvastatin would cause more regression of plaque than simvastatin alone, where plaque was measured by serial IVUS. The primary end point was the change in total and percent atheroma volume (TAV and PAV). Secondary end points were changes in high sensitivity C-reactive protein (hsCRP), matrix metalloproteinase-9 (MMP-9) and soluble CD40 ligand (sCD40L). Patients were randomized to take either niacin 1,000 mg plus simvastatin 40 mg or simvastatin 40 mg alone. Statin or combination therapy was started in both groups immediately after coronary angiography and IVUS. We enrolled a total of 28 patients (14 patients in the combined drug group vs. 14 in the simvastatin alone group) who underwent baseline and follow-up coronary angiography and IVUS. Inclusion criteria were: age 20 to 70, patients who had a mild to moderate degree of coronary stenosis measured by coronary angiogram and who had not been taking cholesterol lowering agents, hormone therapy or anti-oxidant vitamins within the previous 2 months. We excluded premenopausal women, individuals younger than 20 years or older than 70 years, those with hypercholesterolemia (type I, III, IV, V), homozygous familial hypercholesterolemia, those using cholesterol lowering agents (HMG-CoA reductase inhibitors, bile acid sequestrants and nicotinic acid within 6 weeks, fibrate within 8 weeks, probucol within 1 year), the use of cyclosporine or antifungal agents (azole), severe left ventricular dysfunction (an ejection fraction <35%), active liver disease or hepatic dysfunction {alanine aminotransferase (ALT) and aspartate aminotransferase (AST) >20% of the normal value}, renal dysfunction (serum serum creatinine >1.8 mg/dL), hypothyroidism, secondary hypercholesterolemia due to nephrotic syndrome, partial ileal bypass, hypersensitivity to a HMG-CoA reductase inhibitor or an ACE inhibitor and participation in another clinical trial. A mild to moderate degree of coronary stenosis was defined as a stenotic diameter of 30% to 60% of normal, and was assessed by quantitative coronary angiography. After the 9-month treatment period, the patients underwent repeated cardiac catheterizations and IVUS examinations of the matched segments under identical conditions. This study's protocol was approved by the institutional review board of Gil Medical Center, Gachon University of Medicine and Science and informed consent was obtained from all patients.
Methods
Study process
After informed consent was obtained, subjects were randomized (allocation concealed) in a 1 : 1 fashion to receive either niacin 1,000 mg plus simvastatin 40 mg or simvastatin 40 mg alone. Randomization was done with a computer-generated sequence of random numbers. Study medication was initiated at a daily dose of 500 mg for 30 days, which was then increased to 1,000 mg for the duration of the 9-month study period. The study medication was taken at night, and it was recommended that it be taken with the subjects' usual daily dose of anti-anginal medication. All patients taking other medications such as fish-oil more than 200 mg/day, antacid, anticoagulant, immune depressant, corticosteroid, erythromycin, clarithromycin, systemic itraconazole and ketoconazole were strongly encouraged to discontinue their use of these supplements during the study to avoid possible interference with the response to niacin. The authors decided the dose of niacin based on a recent study and the dose of statin based on highest tolerable dose to Koreans.
Laboratory analysis
For all patients, serum samples were collected before coronary angiography for measuring lipid profiles, hs-CRP, blood urea nitrogen (BUN), creatinine, AST andALT. Serum levels of total cholesterol, LDL-C, HDL-C and TG were measured by standard enzymatic methods. hs-CRP was analyzed using commercial kits containing a nephrometry system. MMP-9 and sCD40L were analyzed using commercially available ELISA kits. Serum levels of total cholesterol, LDL-C, HDL-C, TGs, hs-CRP, BUN, creatinine, AST and ALT were measured at baseline and at 9-month follow-up.
Intravascular ultrasound imaging and analysis
Intravascular ultrasound imaging and analysis was done at baseline and at the 9-month follow-up. IVUS examinations were done after intracoronary administration of 200 µg nitroglycerin using a commercially available IVUS system (Boston Scientific Corporation/SCIMed, Minneapolis, MN, USA). The IVUS catheter was advanced distal to the target lesion, and imaging was done retrograde to the aorto-ostial junction at an automatic pullback speed of 0.5 mm/s. The same anatomic image slices were analyzed at baseline and at follow-up. By using axial landmarks (i.e., side branches, calcifications or unusual plaque shapes) and the known pullback speed, identical cross-sectional image slices on serial studies could be identified for making comparisons. We measured IVUS images that were precisely spaced 1 mm apart. The leading edges of the external elastic membrane (EEM) and lumen were traced manually in accordance with the guidelines for IVUS of the American College of Cardiology Clinical Expert Consensus Document on Standards for the Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies.13) The total atheroma volume (TAV) was calculated by summation of the atheroma areas from each measured image: TAV=Σ (the EEM area-the lumen area). The PAV was determined using the formula: PAV= 100×{Σ (the EEM area-the lumen area)/Σ (EEM areas)}.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS) for Windows, version 12.0 (Chicago, IL, USA) was used for all analyses. Continuous variables are presented as mean values±standard deviations (SDs); they were compared using paired or unpaired Student's t-tests or the nonparametric Wilcoxon test if the normality assumption was violated. Discrete variables are presented as percentages and relative frequencies. A repeated measured analysis of variance (ANOVA) test was used for comparing continuous variables before and after treatment. Linear regression analysis was used to evaluate associations between continuous variables. A p<0.05 was considered statistically significant.
Results
Baseline characteristics
There was a total of 28 subjects. Mean age was 60.8±8.0 years in the simvastatin group and 58.1±7.0 years in the niacin/simvastatin group. Seven patients (50%) in the simvastatin group and 7 patients (50%) in the niacin/simvastatin group were males. No patients dropped out because of side effects to niacin or simvastatin. There was no difference in risk factors such as diabetes mellitus, hypertension, smoking and clinical diagnosis between the two groups. Ejection fraction on echocardiograms and results from coronary angiograms were not different between the two groups (Table 1). Laboratory findings between the two groups were not different (Table 2).
Comparison of coronary angiograms and intravascular ultrasound findings between the two groups
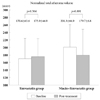
A paired t-test showed no difference in the coronary angiogram or in the IVUS before and after treatment (Table 3). Repeated measured ANOVA adjusted by the initial measurement and changes showed a statistically significant difference. The normalized total atheroma volume (nTAV) before treatment was 170.6±63.6 in the simvastatin group and 201.3±66.9 in niacin/simvastatin group (p=0.364). The nTAV after treatment was 175.9±46.9 in simvastatin group and 179.7±63.8 in the niacin/simvastatin group (p=0.891). Changes in nTAV were significantly different (p=0.024) (Fig. 1) (Table 4). The PAV before treatment was 45.4±9.6 in the simvastatin group and 49.8±10.7 in the niacin/simvastatin group (p=0.407). The PAV after treatment was 44.3±9.9 in the simvastatin group and 48.6±12.4 in the niacin/simvastatin group (p=0.451). Changes in PAV were significantly different (p=0.047) (Figs. 2 and 3) (Table 4).
Comparison of biomarkers of inflammation and oxidative stress between the two groups
After 9 months, hsCRP decreased in the simvastatin group, from 0.661±1.298 mg/dL to 0.341±0.573 mg/dL and decreased in the niacin/simvastatin group from 0.894±1.233 mg/dL to 0.186±0.351 mg/dL (p=0.001) (Fig. 4) (Table 4). After 9 months, MMP-9 increased in the simvastatin group from 10.2±9.8 to 72.5±33.9 and increased in the niacin/simvastatin group from 11.2±6.2 to 84.7±63.3 (p=0.017) (Fig. 5) (Table 4). After 9 months, sCD40L decreased in the simvastatin group from 2,634±1,594 to 961±1,529 and decreased in the niacin/simvastatin group from 2,803±2,033 to 836±1,034 (p<0.001) (Fig. 6) (Table 4).
Discussion
The present study demonstrates that lipid lowering therapy with niacin plus simvastatin induces significant plaque regression and stabilization in angina patients who had a mild to moderate degree of coronary stenosis. The main focus of the present study was to show that the combination of niacin plus simvastatin showed a greater decrease in the TAV and the PAV measured by IVUS, a greater decrease in inflammatory response measured by biomarkers, and a greater decrease in platelet activation as measured by sCD40L (Fig. 7).
Currently, the treatment of lipid abnormalities involves the primary use of statins to reduce serum levels of LDL-C. Multiple studies have shown that statins lower the mortality and morbidity of patients with coronary artery disease and other atherosclerotic vascular diseases.1-4) Statins effectively inhibit mevalonate synthesis and lower LDL-C levels. Beyond lowering the blood lipoprotein level, statins have favorable effects on vascular inflammation,14) endothelial function,15) and plaque regression.16-18) Despite substantial reductions in cardiovascular morbidity and mortality that have been achieved with statins, the protection afforded by these drugs is incomplete. Thus, combination therapies directed at increasing HDL-C are an attractive but unproven approach. This study was the first demonstration of an incremental, independent effect of combination therapy with statin and niacin compared with statin monotherapy to retard the progression of atherosclerosis as measured by IVUS in Korean patients.
Niacin has been in clinical use for 4 decades and is the most effective treatment currently available to increase low levels of HDL-C. The current understanding of its place in an era of potent therapies directed at LDL-C was limited by a lack of studies assessing its incremental effect on atherosclerosis and coronary outcomes. The most recent demonstration of this was the HATS.19) This placebo-controlled study of combined low-dose simvastatin (10 to 20 mg/d) and high dose niacin (2 to 4 mg/d) showed the ability of combination therapy to largely stabilize coronary atherosclerosis with an associated substantial 13% absolute risk reduction (up to 90% relative risk reduction) for cardiovascular outcomes. The absence of a statin monotherapy control group and the use of relatively high doses of niacin, however, limit the capacity to extrapolate the data to a stepwise additive approach to combination therapy in clinical practice that might typically use lower doses of niacin. The data from ARBITER 2 extended our understanding of the potential benefit of combination therapy with statin and niacin in patients with known CHD and moderately low levels of HDL-C beyond multiple previous studies that included niacin as a component of combination therapy.20) ARBITER 2 showed a significant progression of carotid intima media thickness (CIMT) in the placebo (statin monotherapy) group, despite a mean LDL-C of 100 mg/dL, a result that was consistent with previous placebo-controlled studies of statin monotherapy and atherosclerosis progression.11)12)20) Such progression of atherosclerosis in the setting of a statin administered long term differed from the observed initial results of statin administration, likely due to the influence of other lipids (e.g., low HDL-C) and non-lipid risk factors.
Recent data showed that enhanced sCD40L is associated with platelet activation in the setting of hypercholesterolemia, related to an increase in sCD40L to the prothrombotic state previously described in hypercholesterolemia, and provided in vivo evidence that statins might significantly reduce sCD40L and the CD40L-associated prothrombotic state.21) The present study shows that combination therapy of niacin plus simvastatin decreases sCD40L and supports the inhibition of plaque progression.
There is evidence that CRP has proinflammatory and proatherogenic effects via modulation of endothelial, inflammatory and smooth muscle cells of the arterial wall. The proinflammatory, proatherogenic effects of CRP that have been documented in endothelial cells include: 1) decreased nitric oxide and prostacyclin production, and 2) increased production of endothelin-1, cell adhesion molecules, monocyte chemoattractant protein-1, IL-8, and plasminogen activator inhibitor-1.22)23) The present study shows that combination therapy of niacin plus simvastatin decreases hsCRP and explains the inhibition of atherosclerosis progression.
In soft, lipid-rich plaques, especially ones obtained from patients who died of acute coronary syndrome, inflammatory cells including activated macrophages and mast cells accumulate in high concentration. There is an increased rate of formation of MMP enzymes in the ruptured atherosclerotic plaque. Active rupture of the vulnerable plaque by these proteinases is one of the triggers causing subsequent thrombus formation and acute coronary syndrome. This is clinically significant because, serial changes in peripheral blood levels of MMP-2 and MMP-9 were observed in patients with acute coronary syndrome, which implicates a role for these enzymes in the molecular mechanism of plaque destabilization in acute coronary syndrome. Macrophages and smooth muscle cells of human atherosclerotic plaques have been shown to synthesize MMP-3 and MMP-9.24) MMP-9 might directly affect thrombus maturation and dissolution. MMP-9 was able to inhibit platelet aggregation in response to thrombin or collagen 25) and can degrade fibrin.26) Furthermore, thrombus formation can induce MMP-9 release from surrounding cells,27) and MMP-9 knockout mice have an increased propensity to hemorrhage.28) Therefore, MMP-9 can reduce thrombus size, and its increased expression may promote smooth muscle cell-directed healing after atherosclerotic plaque rupture, resulting in retardation of plaque expansion and increased stability of the newly forming cap. Another study showed that MMP-9-dependent processes are activated that initiate a healing response that is involved in the recruitment of smooth muscle cells and in the elaboration of matrix when an acute plaque rupture takes place. Hence, after an acute coronary event, increases in the plasma MMP-9 concentration might be the consequence of a healing response rather than of the initial plaque rupture.29) The present study showed that combination therapy of niacin plus simvastatin increases MMP-9 and explains the plaque stabilization as do the other biomarkers.
The present study has two limitations. First, the study size was relatively small. Second, there was selection bias due to patients being enrolled in a single center. In spite of the limitations, the present study shows two important differences. First, this is the first study, to our knowledge, to show a combined effect of statin and niacin using IVUS parameters in Koreans. Second, the present study shows the additive effect of niacin to high dose statin therapy.
In conclusion, the combination of niacin plus simvastatin reduces TAV and PAV measured by IVUS, reduces inflammatory responses measured by biomarkers and decreases platelet activation measured by sCD40L.









 XML Download
XML Download