

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sustained hypotension without a decrease in inotropic agents is frequently observed after the return of spontaneous circulation (ROSC). The cause of this phenomenon is not fully understood, but several hypotheses have been proposed. Post-ROSC hypotension is characterized by profound myocardial stunning, a systemic pro-inflammatory response, and complicated by persistent precipitating pathologies.1)2) The presence of post-ROSC hypotension is strongly associated with a poor prognosis.3)
Postprandial hypotension (PPH) is a decrease in systolic blood pressure of >20 mm Hg within 2 hours of a meal;4)5) however, PPH has not been described as a cause of post-ROSC hypotension in the intensive care unit (ICU).
We report PPH in a patient who recovered cardiopulmonary resuscitation (CPR) and was treated with acarbose in the ICU.
Case
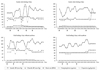
A 74 year old man was admitted to the hospital due to comatose. He had a complicated medical history prior to referral. He had suffered a stroke 10 years ago and was diagnosed with hypertension. He underwent a total gastrectomy due to stomach cancer 2 years ago. Last year, he was diagnosed with ischemic cardiomyopathy and chronic renal failure and has been under continuous medical treatment since that time. On admission, uremic syndrome and pulmonary edema were diagnosed, so he was treated with continuous renal replacement therapy (CRRT). Forty-eight hours after admission, the pulmonary edema had resolved and vital signs had normalized. Anuria improved with the use of diuretics, after which the CRRT was interrupted. He developed sudden monomorphic refractory ventricular tachycardia on the third hospital day (Fig. 1), and CPR was performed for 1 hour. Amiodarone was used to control the ventricular tachycardia. Echocardiographic findings showed an ejection fraction (EF) of 20% (decreased compared to an EF of 40% before CPR, but laboratory studies did not show any abnormal findings). Because of a persistent state of shock after the ROSC, coronary angiography (CAG) was performed. No acute myocardial infarction findings were found. An intra-aortic balloon pump (IABP) was inserted for hemodynamic support and no coronary intervention was performed. The next day his level of consciousness had normalized, and his vital signs (blood pressure, heart rate, and temperature were stable with the use of inotropic agents. The IABP was removed quickly. Amiodarone (1,800 mg) was infused for 24 hours; however, a prolonged QT was observed (QTc, 560 msec); thus, the amiodarone was stopped. Ventilator weaning was difficult because of rib fractures, and gastric tube feeding was started subsequently. The inotropic agents were decreased, and dopamine was decreased to 3 µg/kg/min. Ten days after the ROSC and 3 days after gastric tube feeding, the inotropic agents were increased. The echocardiographic EF (40%) recovered to that seen before CPR. A rapid adrenocorticotropic hormone (ACTH) stimulation test was performed, and the results were normal. Based on the flow sheet, we observed that his blood pressure decreased after meals and that this occurred whether he was fed orally or with a gastric tube (Fig. 2). He complained of dizziness and weakness when the hypotension occurred.
A provocation test was performed the next day, which included ingesting 250 kcal of Jevity® RTH (Abbott, Zwolle, The Netherlands) after an overnight fast. Before ingesting the solution, and up to 90 minutes thereafter, blood glucose, insulin, blood pressure, blood potassium, and heart rate were measured (Table 1). We noted hypotension, but serum hypoglycemia and tachycardia were not observed. The hypotension was diagnosed as PPH. The inotropic agents were discontinued after we chose acarbose for treatment (Fig. 2).6)7)
Discussion
The survival rate is not high among in-hospital CPR cases.8) In the case presented herein, a patient with ROSC began to recover but developed shock for unknown reasons. It has been reported that post-ROSC hypotension is associated with a poor prognosis.3) Therefore, any cause of hypotension should be identified and treated. The direct causes of post-ROSC hypotension are myocardial dysfunction, systemic reperfusion response, and a persistent precipitating pathology.1) However, these were not the cause of the hypotension in this case. The left ventricular EF recovered to the level prior to CPR, and because the rapid ACTH stimulation test result was normal, the cause of the shock was not adrenal insufficiency. No evidence of an inflammatory reaction was found. PPH was suspected when searching for other causes of hypotension after reviewing the flow sheet.
PPH is defined as a decrease in systolic blood pressure of >20 mm Hg within 2 hours of the start of a meal.4)5) However, this patient had undergone a gastrectomy; thus, PPH needed to be distinguished from dumping syndrome. Although the pathophysiology of elderly PPH and dumping syndrome is unclear, there are differences in clinical presentations. The pathophysiology of dumping syndrome is excess secretion of gastrointestinal (GI) peptides and insulin as a result of a fluid shift in the small bowel.9) However, the pathophysiology of elderly PPH can be explained by inadequate sympathetic nervous system compensation for meal-induced splanchnic blood pooling, impaired baroreflex function, inadequate post-prandial increases in cardiac output, impaired peripheral vasoconstriction, insulin-induced vasodilatation, and release of vasodilatory GI peptides.1)10) Therefore, elderly PPH does not result in tachycardia or hypoglycemia when compared to dumping syndrome. This patient had the same clinical features, so PPH was more likely than dumping syndrome.
In Korea, the incidence of elderly PPH tends to be high,11)12) and elderly patients with PPH have a high mortality rate.13) Therefore, it is important to diagnose and treat PPH.
Many medications have been considered for treating PPH, most of which increase blood pressure.4) A recent study showed that acarbose is the most effective treatment for PPH.7) Considering that the patient's fasting glucose was 125 mg/dL, we prescribed acarbose and stopped inotropic agents completely.
In summary, this is the first case in which post-ROSC hypotension was treated with acarbose for PPH. Post-ROSC hypotension is strongly associated with a poor prognosis,3) and elderly patients with PPH have a high mortality rate.13) Therefore, PPH should be considered and treated to manage hypotension in elderly patients in the ICU.


 XML Download
XML Download