

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Anorexia nervosa (AN) is characterized by a decrease in caloric intake, weight loss, amenorrhea and behavioral changes. According to Morris and Twaddle,1) eighty percent of AN patients have cardiovascular complications, such as bradycardia, hypotension, arrhythmia and repolarization abnormalities, and ten percent of them experience sudden cardiac death. Stress-induced cardiomyopathy (SICMP) is designated after echocardiographic abnormalities that are characterized by extensive akinesia (ballooning) of the apical region and hypercontraction of the basal segment of the left ventricle (LV).2) Patients with SICMP demonstrate cardiac enzyme abnormalities and electrocardiographic (ECG) changes similar to those seen in acute myocardial infarction (MI) without significant luminal narrowing of the coronary arteries on the coronary angiography.3) SICMP is a very rare complication of AN. We report a rare case of SICMP caused by separation anxiety as a precipitating event in AN.
Case
A 35-year-old woman came to our emergency department complaining of severe general weakness and epigastric pain for the last 5 days. In her past medical history, she was diagnosed with AN and borderline personality disorder at a local psychiatric clinic 5 years ago. The only meals she used to have on a daily basis were milk and fruits for a period of 17 years, and even her daily meal intake rapidly decreased after her mother went abroad two weeks ago. This was because she appeared to be extremely dependent on her mother. She did not have any history of diabetes mellitus, hypertension, or hepatitis previously. However, she had taken psychiatric medications for 6 months approximately 5 years ago. In addition, she also intermittently took medications for amenorrhea and osteoporosis.
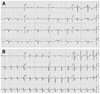
On admission, her vital signs were: blood pressure of 90/60 mm Hg, pulse rate of 60 beats/min, respiration rate of 20 breaths/min, and body temperature of 36.5℃. She was alert, but looked chronically ill and cachexic. Her body weight was 30 kg and body mass index was 11.71 kg/m2. She had a severely dehydrated tongue, but her chest and abdomen physical examination showed no abnormalities. Her laboratory examinations were as follows; white blood cell 8,940/mm3, hemoglobin 15.8 g/dL, hematocrit 43.8%, platelet 70,000/mm3, random blood glucose 132 mg/dL, blood urea nitrogen/creatinine 35.9/0.44 mg/dL, total protein/albumin 5.6/3.6 g/dL, aspartate aminotransferase/alanine aminotransferase 471/374 IU/L, total bilirubin 1.90 mg/dL, Na/K 127/2.6 mEq/L, Ca/P/Mg 8.5/5.3/1.6 mg/dL, total cholesterol 116 mg/dL, triglyceride 38 mg/dL, high density lipoprotein-cholesterol 74 mg/dL, low density lipoprotein-cholesterol <10 mg/dL, T3 0.43 ng/mL (0.78-1.82 ng/mL), free T4 0.94 ng/mL (0.85-1.86 ng/mL), thyroid stimulating hormone 1.71 mIU/L (0.17-4.05 mIU/L), adrenocoticotropic hormone 11.44 pg/mL (6.00-56.70 pg/mL), cortisol 17.40 ug/dL (9.41-26.06 ug/dL), and aldosterone 31.66 pg/mL (40-102 pg/mL). Initial cardiac biomarkers were elevated as follows; creatine kinase-MB 154.30 ng/mL (0-5 ng/mL), troponin-I 2.580 ng/mL (0-0.78 ng/mL) and N-terminal pro-B-type natriuretic peptide 8,963 pg/mL (0-155 pg/mL). Her chest X-ray and abdomen computed tomography showed no significant lesions associated with epigastic pain. Initial electrocardiogram showed sinus rhythm (60 beats/min), prolonged corrected QT interval (543 ms), pathologic Q waves in II, III, aVF and V1-V3, inverted T waves in II, III and aVF and poor R progression in precordial leads (Fig. 1A). Echocardiogram revealed large akinetic areas around the apical, inferior, anterior and lateral sides with hypercontraction of the basal segments, linear echogenic mural thrombus, pericardial effusion, and a reduction of ejection fraction to 36% (Fig. 2). Therefore, we strongly suspected that she was SICMP because of her characteristic echocardiograhic findings.
Only standard medical treatment was given to the patient since she and her guardian refused to receive a coronary angiogram. Therefore, we started the treatment with low molecular weight heparin, and nutrition support with immediate multi-systemic interventions. Psychiatric consultation was also accompanied by medical therapy. After three days, we stopped anticoagulation therapy due to aggravated thrombocytopenia and prolonged prothrombin time (PT). Overall, her daily oral intake increased together with her body weight, 33 kg compared to 30 kg in the beginning. Electrolyte imbalance, liver dysfunction, and thrombocytopenia were also normalized. Two weeks later, the next follow-up echocardiogram indicated a significant improvement of the LV ejection fraction (42%) and wall motion abnormalities. On the other hand, apical mural thrombosis still remained and pericardial effusion increased (Fig. 3). On the next follow-up electrocardiogram, the corrected QT interval decreased to 453 ms. Furthermore, pathologic Q waves, inverted T waves and poor R progression observed in the initial ECG disappeared (Fig. 1B). However, she and her guardian strongly insisted on discharging from the hospital against the clinician's recommendation. Although appointments with cardiology and psychiatry departments were arranged with continuing mental support and follow-up echocardiogram, she never came back to the hospital after her discharge.
Discussion
AN is characterized by a decrease in caloric intake, weight loss, amenorrhea and behavioral changes. Most AN patients are adolescents with a mean age of 15 years old.1) Patients with AN may also suffer from bone marrow suppression, liver failure and numerous metabolic complications, and it is assumed that these complications are caused by severe malnutrition.4) Eighty percent of these patients have cardiovascular complications, such as bradycardia, hypotension, arrhythmia and repolarization abnormalities.5) Furthermore, 10% of them experience sudden cardiac death.6) Myocardial mass decreases together with body weight, and results in a reduction in LV ejection fraction and diffuse global wall motion abnormalities. Myocardial damage is reversible with a tolerable prognosis since body weight can be regained.7)
SICMP is characterized by a transient mid ventricular dysfunction and apical akinesis, diskinesis with the basal function preserved, or hyperkinetic. The latter is a rare case of AN only found in a few case reports.8)9) Some patients with SICMP are complicated with mural thrombosis as seen in acute MI. According to Haghi et al.10) 8% of SICMP patients had mural thrombosis in the LV. However, patients who have SICMP with mural thrombosis have not ever been reported in Korea. In our study, low molecular weight heparin was infused after admission, and on the third day, anticoagulant therapy had to be halted because of no improvement of thrombocytopenia and PT prolongation. Only intravenous nutritional support and correction of electrolyte imbalance were sustained.
Recurrence rate of SICMP with a precipitant as psychiatric disorder is supposed to be higher than that of previously published data,11-13) because physical or emotional stress related to the psychiatric disorder is not transient. Treatment of SICMP especially in AN patients who also suffer from other complications after severe malnutrition should be investigated with multi-systemic approaches.


 XML Download
XML Download