

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute myocardial infarction (AMI) is a rare complication that can occur after blunt chest trauma.1)2) Blunt chest trauma can lead to various cardiac complications ranging from nonsignificant arrhythmias to myocardial rupture.1) A variety of injuries to the coronary arteries, including laceration, thrombosis, intimal dissection, arteriovenous fistula and pseudoaneurysm formation following blunt trauma have been rarely reported.1) We report a case of a 33-year-old male who sustained a blunt chest trauma in a traffic accident resulting in left ventricular (LV) thrombus with distal embolization due to AMI caused by occlusion of the ostium of left anterior descending artery (LAD).
Case
A 33-year-old man without known medical problems was admitted to the hospital because of abrupt onset of claudication in the left lower extremity with associated color changes in the left foot. He had no risk factor for ischemic heart disease except for current smoking. He had sustained blunt chest trauma due to hitting the steering wheel in a traffic accident about 4 years ago. At that time, he was treated conservatively for rib fracture without performing any cardiac examinations in a small orthopaedic clinic. After that incident, he had dyspnea on exertion and chest tightness during exercise. However, he did not think it was serious and hence did not undergo any further medical evaluation.
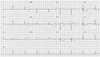
On physical examination, his blood pressure was 110/60 mmHg, heart rate 70 beats per minute. Auscultation of the heart revealed a regular rhythm without significant murmurs or abnormal heart sounds. The cardiac enzyme profile and other routine laboratory tests were within normal ranges. The initial electrocardiogram showed poor R wave progression and ischemic T wave abnormality in leads V2-V5 (Fig. 1).
On admission, the peripheral angiography showed total occlusion of the left popliteal artery (Fig. 2). The echocardiography and MRI revealed a LV thrombus measuring 3.98×1.74 cm in size, and aneurysmal change of the LV apex, and akinesia of the anterior and anteroseptal segments from base to apex (Fig. 3). Coronary angiography revealed total occlusion of the ostium of the LAD (Fig. 4). Intravascular ultrasound (IVUS) was not performed since the guidewire failed to pass the coronary lesion. Popliteal artery endarterectomy and coronary artery bypass graft (CABG) with LV thrombectomy were performed successfully without complications. The pathological diagnosis of the LV specimen was fibrinous blood clots (Fig. 5).
Discussion
Blunt chest trauma can cause various cardiac complications ranging from supraventricular arrhythmia to valvular and myocardial rupture. Injury to coronary arteries is rare, but is associated with a significant risk of mortality from AMI.1-3) The proposed causes of AMI following blunt chest trauma include a variety of injuries to the coronary arteries, such as laceration, thrombosis, intimal dissection, arteriovenous fistula and pseudoaneurysm.1) Thrombosis has been the main suspect in pathogenesis of coronary occlusion following trauma.1)8)10)
The mechanism of myocardial infarction after a blunt chest trauma involves shearing forces applied to the coronary artery, which cause intimal tearing. The intimal injury in turn precipitates platelet aggregation and intracoronary thrombosis.7) Compression of the anterior chest wall and shear forces in the arterial wall generated by sudden deceleration during traumatic impact are presumed to be responsible for the arterial injury.6)
The LAD is the most frequently injured vessel, followed by the right coronary, and the circumflex artery is the least commonly involved vessel.8-10) The higher incidence of LAD involvement may be due to its proximity to the chest wall. The possibility that preexisting atherosclerotic plaque may predispose the vessel wall to a traumatic disruption at that site has been suggested.7)
IVUS provides a cross-sectional view of a specific portion of the vasculature. This information could be used to determine the most suitable strategy to treat unusual coronary artery disease.10) Moreover, it is possible to overcome the limited ability of angiography in assessing the disease mechanism using IVUS. The previous reports of IVUS findings in traumatic myocardial infarction suggest that intimal dissection at the ostium of the LAD with preexisting intermediate lesion resulting from chest trauma could be the cause of thrombotic occlusion and myocardial infarction.7) In our case, we did not perform IVUS since guidewire passage was not possible. Hence, we could not obtain coronary arterial anatomical images using IVUS. Even if we had obtained the IVUS images, it might not have been a typical coronary artery dissection image or other pathological images due to chronic remodeling of the vessel.
In several cases, coronary artery dissection may heal spontaneously with a few exceptions such as this case.5)10)11) In addition, during the acute phase, the management of patients with multiple blunt chest trauma using thrombolytic therapy is controversial, because it may worsen the dissection itself and increase the bleeding risk.4) Emergency CABG also has reported good results in some adequate cases, but such a major operation can be accompanied by an increased risk of post-operative complications in patients with multiple trauma.12) The myocardial scintigraphy, which reveals the viability of myocardium, may help in proper clinical decision making regarding the intervention.
In conclusion, when patients with chest trauma exhibit symptoms and electrocardiographic changes suggestive of ischemic heart disease, immediate coronary angiography should be considered and further management may depend on the angiography findings.




 XML Download
XML Download